Floberg John M, Wells Shane A, Ojala Diane, Bayliss R Adam, Hill Patrick M, Morris Brett A, Morris Zachary S, Ritter Mark, Cho Steve Y
Departments of Human Oncology.
Radiology, University of Wisconsin, Madison, Wisconsin.
Adv Radiat Oncol. 2023 Apr 9;8(5):101241. doi: 10.1016/j.adro.2023.101241. eCollection 2023 Sep-Oct.
The recently reported FLAME trial demonstrated a biochemical disease-free survival benefit to using a focal intraprostatic boost to multiparametric magnetic resonance imaging (mpMRI)-identified lesions in men with localized prostate cancer treated with definitive radiation therapy. Prostate-specific membrane antigen (PSMA)-directed positron emission tomography (PET) may identify additional areas of disease. In this work, we investigated using both PSMA PET and mpMRI in planning focal intraprostatic boosts using stereotactic body radiation therapy (SBRT).
We evaluated a cohort of patients (n = 13) with localized prostate cancer who were imaged with 2-(3-(1-carboxy-5-[(6-[18F]fluoro-pyridine-2-carbonyl)-amino]-pentyl)-ureido)-pentanedioic acid (F-DCFPyL) PET/MRI on a prospective imaging trial before undergoing definitive therapy. The number of lesions concordant (overlapping) and discordant (no overlap) on PET and MRI was assessed. Overlap between concordant lesions was evaluated using the Dice and Jaccard similarity coefficients. Prostate SBRT plans were created fusing the PET/MRI imaging to computed tomography scans acquired the same day. Plans were created using only MRI-identified lesions, only PET-identified lesions, and the combined PET/MRI lesions. Coverage of the intraprostatic lesions and doses to the rectum and urethra were assessed for each of these plans.
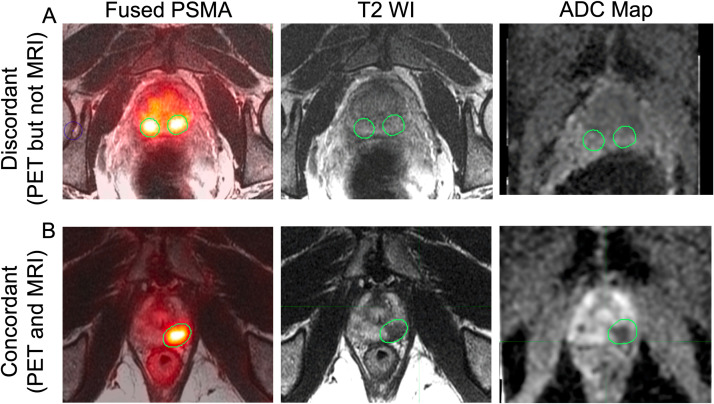
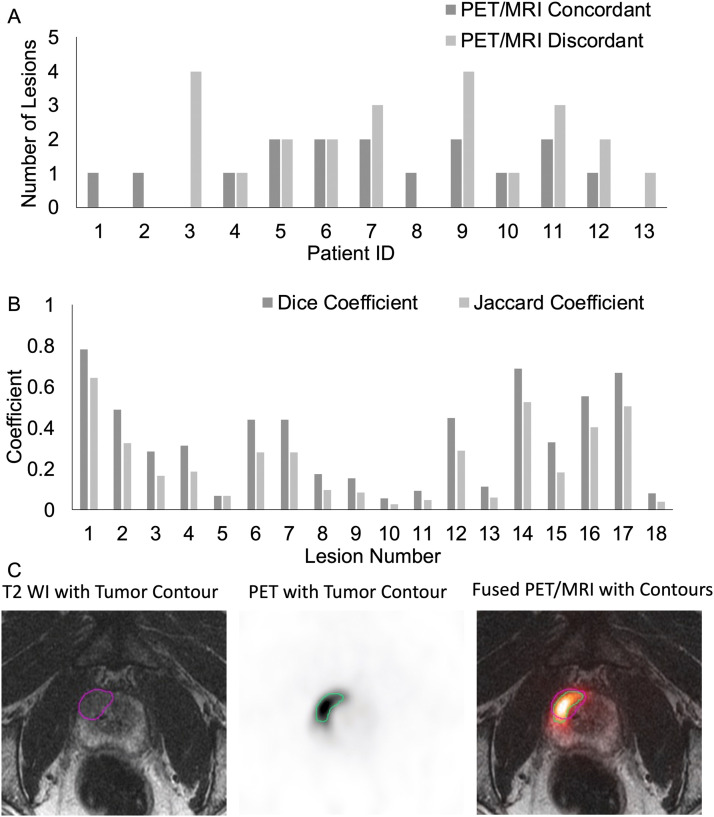
The majority of lesions (21/39, 53.8%) were discordant between MRI and PET, with more lesions seen by PET alone (12) than MRI alone (9). Of lesions that were concordant between PET and MRI, there were still areas that did not overlap between scans (average Dice coefficient, 0.34). Prostate SBRT planning using all lesions to define a focal intraprostatic boost provided the best coverage of all lesions without compromising constraints on the rectum and urethra.
Using both mpMRI and PSMA-directed PET may better identify all areas of gross disease within the prostate. Using both imaging modalities could improve the planning of focal intraprostatic boosts.
最近报道的FLAME试验表明,对于接受根治性放射治疗的局限性前列腺癌男性患者,对多参数磁共振成像(mpMRI)识别出的病变进行前列腺内局部加量放疗可带来无生化疾病生存获益。前列腺特异性膜抗原(PSMA)导向的正电子发射断层扫描(PET)可能会识别出更多的疾病区域。在本研究中,我们探讨了在使用立体定向体部放射治疗(SBRT)计划前列腺内局部加量放疗时同时使用PSMA PET和mpMRI的情况。
我们评估了一组局限性前列腺癌患者(n = 13),这些患者在接受根治性治疗前参加了一项前瞻性成像试验,接受了2-(3-(1-羧基-5-[(6-[18F]氟吡啶-2-羰基)-氨基]-戊基)-脲基)-戊二酸(F-DCFPyL)PET/MRI检查。评估了PET和MRI上一致(重叠)和不一致(无重叠)病变的数量。使用Dice和Jaccard相似系数评估一致病变之间的重叠情况。将PET/MRI成像与同一天采集的计算机断层扫描融合,创建前列腺SBRT计划。分别使用仅MRI识别的病变、仅PET识别的病变以及PET/MRI联合识别的病变创建计划。评估这些计划中前列腺内病变的覆盖情况以及直肠和尿道所接受的剂量。
大多数病变(21/39,53.8%)在MRI和PET之间不一致,单独PET发现的病变(12个)比单独MRI发现的病变(9个)更多。在PET和MRI一致的病变中,扫描之间仍有未重叠的区域(平均Dice系数为0.34)。使用所有病变来定义前列腺内局部加量放疗的前列腺SBRT计划能在不影响对直肠和尿道限制的情况下,提供对所有病变的最佳覆盖。
同时使用mpMRI和PSMA导向的PET可能能更好地识别前列腺内所有大体疾病区域。使用这两种成像方式可改善前列腺内局部加量放疗的计划。