Sánchez Fructuoso Ana I, Bedia Raba Andrea, Banegas Deras Eduardo, Vigara Sánchez Luis A, Valero San Cecilio Rosalía, Franco Esteve Antonio, Cruzado Vega Leonidas, Gavela Martínez Eva, González Garcia María E, Saurdy Coronado Pablo, Morales Nancy D Valencia, Zarraga Larrondo Sofía, Ridao Cano Natalia, Mazuecos Blanca Auxiliadora, Hernández Marrero Domingo, Beneyto Castello Isabel, Paul Ramos Javier, Sierra Ochoa Adriana, Facundo Molas Carmen, González Roncero Francisco, Torres Ramírez Armando, Cigarrán Guldris Secundino, Pérez Flores Isabel
Nephrology Department, Hospital Clínico San Carlos IdSSC, Complutense University, Madrid, Spain.
Nephrology Department, Hospital de Cruces, Bilbao, Spain.
Clin Kidney J. 2023 Jan 11;16(6):1022-1034. doi: 10.1093/ckj/sfad007. eCollection 2023 Jun.
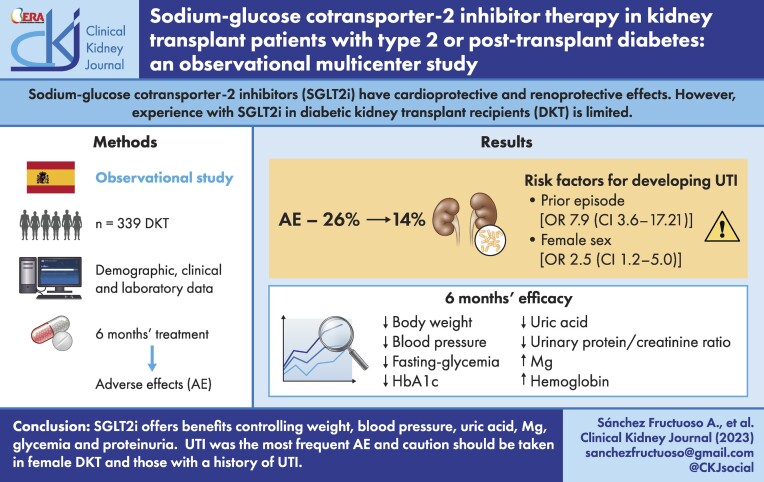
Sodium-glucose cotransporter-2 inhibitors (SGLT2is) have cardioprotective and renoprotective effects. However, experience with SGLT2is in diabetic kidney transplant recipients (DKTRs) is limited.
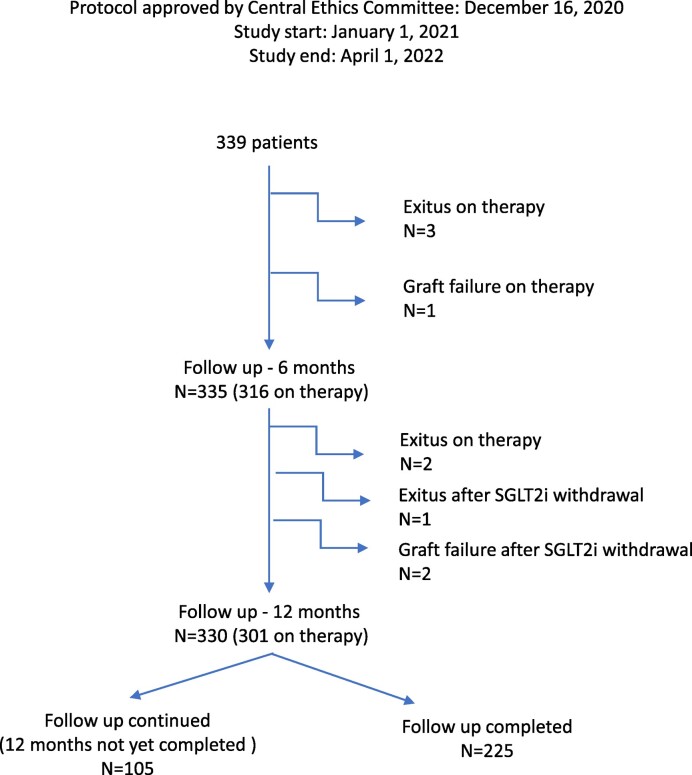
This observational multicentre study was designed to examine the efficacy and safety of SGLT2is in DKTRs. The primary outcome was adverse effects within 6 months of SGLT2i treatment.
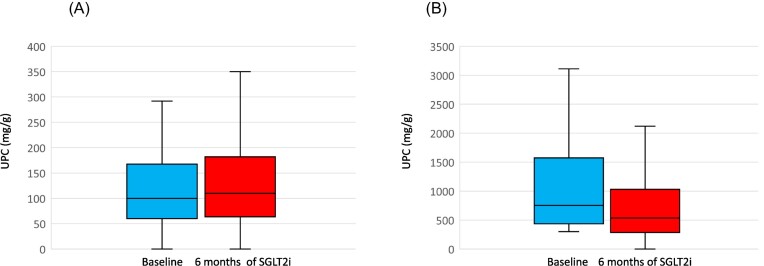
Among 339 treated DKTRs, adverse effects were recorded in 26%, the most frequent (14%) being urinary tract infection (UTI). In 10%, SGLT2is were suspended mostly because of UTI. Risk factors for developing a UTI were a prior episode of UTI in the 6 months leading up to SGLT2i use {odds ratio [OR] 7.90 [confidence interval (CI) 3.63-17.21]} and female sex [OR 2.46 (CI 1.19-5.03)]. In a post hoc subgroup analysis, the incidence of UTI emerged as similar in DKTRs treated with SGLT2i for 12 months versus non-DKTRs (17.9% versus 16.7%). Between baseline and 6 months, significant reductions were observed in body weight [-2.22 kg (95% CI -2.79 to -1.65)], blood pressure, fasting glycaemia, haemoglobin A1c [-0.36% (95% CI -0.51 to -0.21)], serum uric acid [-0.44 mg/dl (95% CI -0.60 to -0.28)] and urinary protein:creatinine ratio, while serum magnesium [+0.15 mg/dl (95% CI 0.11-0.18)] and haemoglobin levels rose [+0.44 g/dl (95% CI 0.28-0.58]. These outcomes persisted in participants followed over 12 months of treatment.
SGLT2is in kidney transplant offer benefits in terms of controlling glycaemia, weight, blood pressure, anaemia, proteinuria and serum uric acid and magnesium. UTI was the most frequent adverse effect. According to our findings, these agents should be prescribed with caution in female DKTRs and those with a history of UTI.
钠-葡萄糖协同转运蛋白2抑制剂(SGLT2i)具有心脏保护和肾脏保护作用。然而,SGLT2i在糖尿病肾移植受者(DKTR)中的应用经验有限。
本观察性多中心研究旨在探讨SGLT2i在DKTR中的疗效和安全性。主要结局是SGLT2i治疗6个月内的不良反应。
在339例接受治疗的DKTR中,26%记录到不良反应,最常见的(14%)是尿路感染(UTI)。10%的患者中,SGLT2i大多因UTI而停用。发生UTI的危险因素是在开始使用SGLT2i前6个月内有UTI病史{比值比[OR]7.90[置信区间(CI)3.63 - 17.21]}以及女性[OR 2.46(CI 1.19 - 5.03)]。在一项事后亚组分析中,接受SGLT2i治疗12个月的DKTR与非DKTR的UTI发生率相似(17.9%对16.7%)。在基线至6个月期间,观察到体重显著下降[-2.22 kg(95%CI -2.79至-1.65)]、血压、空腹血糖、糖化血红蛋白A1c[-0.36%(95%CI -0.51至-0.21)]、血清尿酸[-0.44 mg/dl(95%CI -0.60至-0.28)]以及尿蛋白:肌酐比值下降,而血清镁[+0.15 mg/dl(95%CI 0.11 - 0.18)]和血红蛋白水平上升[+0.44 g/dl(95%CI 0.28 - 0.58)]。这些结果在接受12个月以上治疗的参与者中持续存在。
肾移植中使用SGLT2i在控制血糖、体重、血压、贫血、蛋白尿以及血清尿酸和镁方面具有益处。UTI是最常见的不良反应。根据我们的研究结果,在女性DKTR和有UTI病史的患者中应谨慎使用这些药物。