School of Allied Health Sciences, Department of Health Information Management. University Post Office, University of Cape Coast, Cape Coast, Ghana.
Department of Epidemiology, Biostatistics and Disease Control, University for Development Studies, Tamale, Ghana.
BMC Health Serv Res. 2023 Jun 1;23(1):567. doi: 10.1186/s12913-023-09584-4.
The availability of low-cost computing and digital telecommunication in the 1980s made telehealth practicable. Telehealth has the capacity to improve healthcare access and outcomes for patients while reducing healthcare costs across a wide range of health conditions and situations.
This study compares the adoption, advantages, and challenges of telehealth services between high-income (HICs) and low-and-middle-income countries (LMICs) before and during the COVID-19 pandemic.
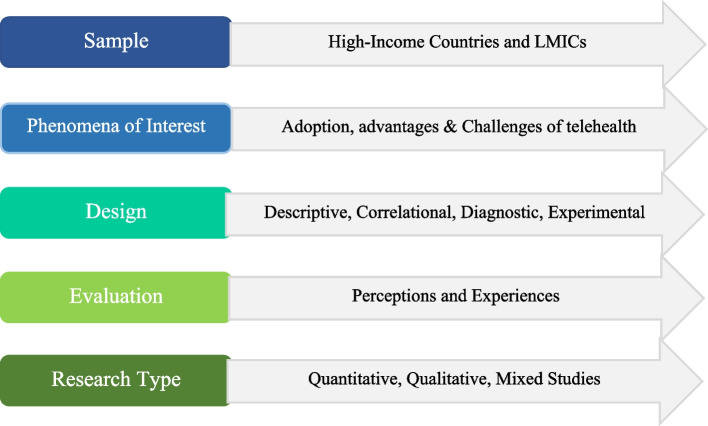
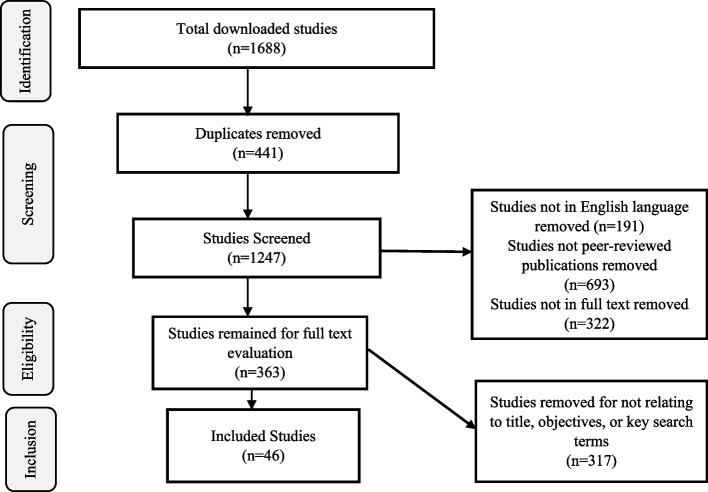
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed. The key search terms were: "Telehealth", "Telehealth in HICs", "Telehealth in LMICs", "Telehealth before COVID-19", "Telehealth during COVID-19". We searched exhaustively ProQuest, Scopus, Web of Science, Google Scholar, CINAHL, and EMBASE databases from 2012. Booleans OR/AND were combined with key search terms to increase relevant search results. The literature search and selection process followed the Sample, Phenomena of Interest, Design, Evaluation, and Research (SPIDER) question format.
The adoption of telehealth before COVID-19 was generally low in both HICs and LMICs. The impact of COVID-19 accelerated the adoption of telehealth at the facility level but not nationwide in both high-income countries and LMICs. The rapid adoption of telehealth at the facility level in both high-income and LMICs introduced several challenges that are unique to each country and need to be addressed.
The lack of national policies and regulations is making the adoption of telehealth at the national level challenging in both high and low-middle-income countries. Governments and Stakeholders of healthcare must consider telehealth as a healthcare procedure that should be deployed in clinical working procedures. Primary quantitative and qualitative studies must be conducted to address challenges encountered during the pilot implementation of telehealth services in both high-income countries and LMICs before and during pandemics.
20 世纪 80 年代,廉价计算和数字电信技术的出现使远程医疗成为可能。远程医疗有能力改善患者的医疗服务获取和结果,同时降低广泛的健康状况和情况下的医疗成本。
本研究比较了高收入国家(HICs)和中低收入国家(LMICs)在 COVID-19 大流行之前和期间采用远程医疗服务的情况、优势和挑战。
遵循系统评价和荟萃分析的首选报告项目(PRISMA)指南。关键搜索词是:“远程医疗”、“HICs 的远程医疗”、“LMICs 的远程医疗”、“COVID-19 之前的远程医疗”、“COVID-19 期间的远程医疗”。我们从 2012 年开始全面搜索 ProQuest、Scopus、Web of Science、Google Scholar、CINAHL 和 EMBASE 数据库。布尔运算符“OR/AND”与关键搜索词结合使用,以增加相关搜索结果。文献检索和选择过程遵循样本、感兴趣现象、设计、评估和研究(SPIDER)问题格式。
在 COVID-19 大流行之前,远程医疗的采用在高收入国家和中低收入国家都普遍较低。COVID-19 的影响加速了设施层面远程医疗的采用,但在高收入国家和中低收入国家都没有全国范围内的采用。在高收入国家和中低收入国家,设施层面远程医疗的快速采用带来了一些独特的挑战,需要加以解决。
高收入和中低收入国家在国家层面采用远程医疗面临的挑战是缺乏国家政策和法规。政府和医疗保健利益相关者必须将远程医疗视为一种应在临床工作流程中部署的医疗程序。必须在高收入国家和中低收入国家之前和期间大流行期间,在试点实施远程医疗服务时遇到的挑战,进行主要的定量和定性研究。