Department of Orthopaedic, Trauma, and Reconstructive Surgery, RWTH University Hospital, Pauwelsstraße 30, 52074, Aachen, Germany.
Department of Orthopedics and Trauma Surgery, Academic Hospital of Bolzano (SABES-ASDAA), 39100, Bolzano, Italy.
Arch Orthop Trauma Surg. 2023 Oct;143(10):6273-6282. doi: 10.1007/s00402-023-04933-8. Epub 2023 Jun 7.
Inside-out and all-inside arthroscopic meniscal repairs are widely performed. However, it remains unclear which method promotes greater clinical outcomes. This study compared inside-out versus all-inside arthroscopic meniscal repair in terms of patient-reported outcome measures (PROMs), failures, return to play, and symptoms.
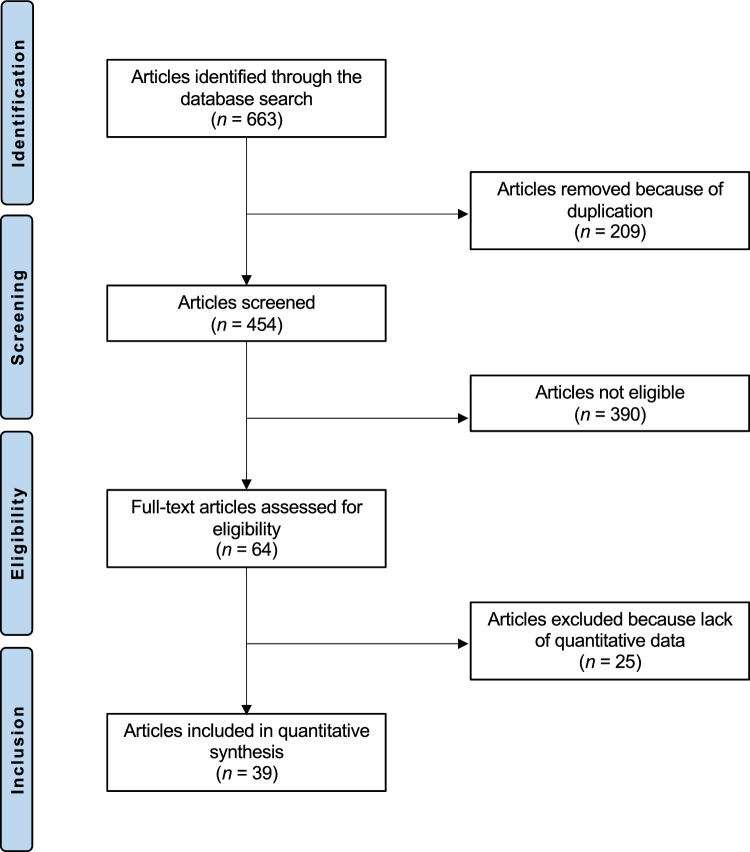
This systematic review was conducted in accordance with the PRISMA guidelines. Two authors independently performed the literature search by accessing the following databases: PubMed, Google Scholar, and Scopus in February 2023. All clinical studies which investigated the outcomes of all-inside and/or inside-out meniscal repair were considered.
Data from 39 studies (1848 patients) were retrieved. The mean follow-up was 36.8 (9 to 120) months. The mean age of the patients was 25.8 ± 7.9 years. 28% (521 of 1848 patients) were women. No difference was found in PROMs: Tegner Activity Scale (P = 0.4), Lysholm score (P = 0.2), and International Knee Document Committee score (P = 0.4) among patients undergoing meniscal repair with all inside or inside-out techniques. All-inside repairs showed a greater rate of re-injury (P = 0.009) but also a greater rate of return to play at the pre-injury level (P = 0.0001). No difference was found in failures (P = 0.7), chronic pain (P = 0.05), reoperation (P = 0.1) between the two techniques. No difference was found in the rate of return to play (P = 0.5) and to daily activities (P = 0.1) between the two techniques.
Arthroscopic all-inside meniscal repair may be of special interest in patients with a particular interest in a fast return to sport, while, for less demanding patients, the inside-out suture technique may be recommended. High-quality comparative trials are required to validate these results in a clinical setting.
Level III, systematic review.
关节镜下半月板内、外缝合修复术被广泛应用。然而,哪种方法能带来更好的临床效果仍不清楚。本研究比较了关节镜下半月板内、外缝合修复术在患者报告的结局指标(PROMs)、失败率、重返运动和症状方面的差异。
本系统评价按照 PRISMA 指南进行。两位作者于 2023 年 2 月通过访问 PubMed、Google Scholar 和 Scopus 等数据库,独立进行文献检索。纳入所有比较关节镜下内、外缝合半月板修复术结局的临床研究。
共检索到 39 项研究(1848 例患者)的数据。平均随访时间为 36.8(9 至 120)个月。患者的平均年龄为 25.8±7.9 岁。28%(1848 例患者中有 521 例)为女性。在接受半月板内、外缝合修复术的患者中,PROMs 无差异:Tegner 活动量表(P=0.4)、Lysholm 评分(P=0.2)和国际膝关节文献委员会评分(P=0.4)。全内修复组再损伤率更高(P=0.009),但重返术前运动水平的比例也更高(P=0.0001)。两种技术的失败率(P=0.7)、慢性疼痛(P=0.05)和再手术率(P=0.1)无差异。两种技术在重返运动(P=0.5)和日常活动(P=0.1)的比例无差异。
关节镜全内半月板修复术可能特别适用于对快速重返运动有特殊兴趣的患者,而对于要求较低的患者,可推荐采用关节镜外缝合技术。需要高质量的对照试验来验证这些结果在临床环境中的有效性。
III 级,系统评价。