Department of Emergency Medicine.
Department of Intensive Care.
Eur J Emerg Med. 2023 Oct 1;30(5):324-330. doi: 10.1097/MEJ.0000000000001042. Epub 2023 Jun 8.
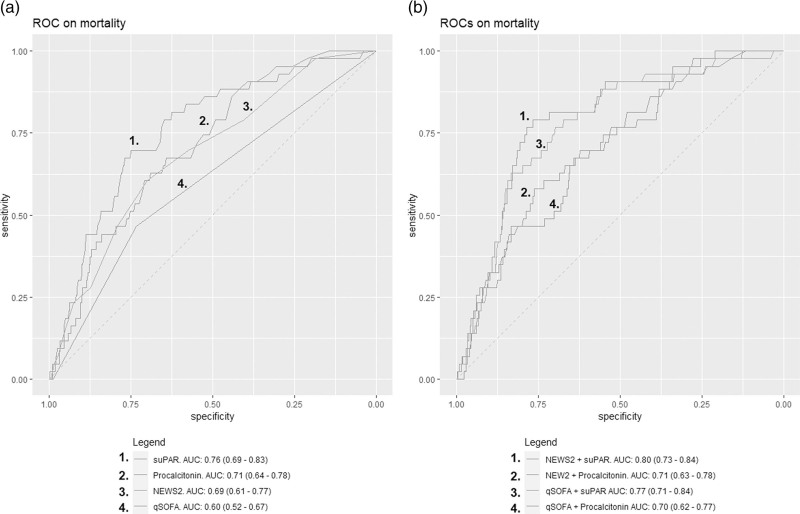
Early identification of patients at risk of clinical deterioration may improve prognosis of infected patients in the emergency department (ED). Combining clinical scoring systems with biomarkers may result in a more accurate prediction of mortality than a clinical scoring system or biomarker alone.
The objective of this study is to investigate the performance of the combination of National Early Warning Score-2 (NEWS2) and quick Sequential Organ Failure Assessment (qSOFA) score with soluble urokinase plasminogen activator receptor (suPAR) and procalcitonin to predict 30-day mortality in patients with a suspected infection in the ED.
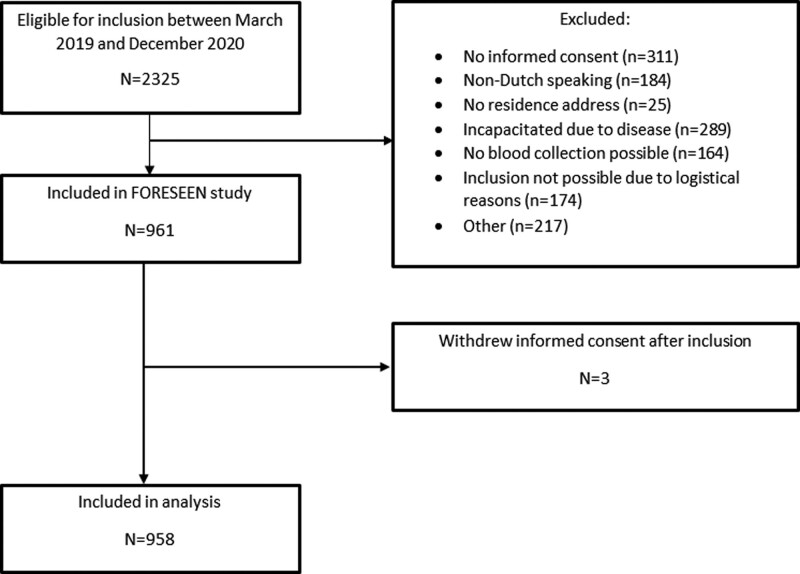
DESIGN, SETTINGS AND PARTICIPANTS: This was a single-center prospective observational study, conducted in the Netherlands. Patients with suspected infection in the ED were included in this study and followed-up for 30 days. The primary outcome of this study was all cause 30-day mortality. The association between suPAR and procalcitonin with mortality was assessed in subgroups of patients with low and high qSOFA (<1 and ≥1) and low and high NEWS2 (<7 and ≥7).
Between March 2019 and December 2020, 958 patients were included. A total of 43 (4.5%) patients died within 30 days after ED visit. A suPAR ≥ 6 ng/ml was associated with an increased mortality risk: 5.5 vs. 0.9% ( P < 0.01) in patients with qSOFA = 0 and 10.7 vs. 2.1% ( P = 0.02) in patients with qSOFA ≥ 1. There was also an association between procalcitonin ≥0.25 ng/ml and mortality: 5.5 vs. 1.9% ( P = 0.02) for qSOFA = 0 and 11.9 vs. 4.1% ( P = 0.03) for qSOFA ≥ 1. Similar associations were found within patients with a NEWS < 7 (5.9 vs. 1.2% for suPAR and 7.0 vs. 1.7% for procalcitonin, P < 0.001).
In this prospective cohort study, suPAR and procalcitonin were associated with increased mortality in patients with either a low or high qSOFA and patients with low NEWS2.
早期识别有临床恶化风险的患者可能会改善急诊科(ED)感染患者的预后。将临床评分系统与生物标志物相结合,可能比单独使用临床评分系统或生物标志物更能准确预测死亡率。
本研究旨在探讨新型预警评分-2(NEWS2)和快速序贯器官衰竭评估(qSOFA)评分与可溶性尿激酶型纤溶酶原激活物受体(suPAR)和降钙素原联合预测疑似感染患者 ED 30 天死亡率的性能。
设计、地点和参与者:这是一项在荷兰进行的单中心前瞻性观察性研究。本研究纳入了疑似 ED 感染的患者,并对其进行了 30 天的随访。本研究的主要结局是全因 30 天死亡率。在 qSOFA(<1 和≥1)和 NEWS2(<7 和≥7)低值和高值亚组中,评估了 suPAR 和降钙素原与死亡率之间的相关性。
2019 年 3 月至 2020 年 12 月期间,共纳入 958 例患者。共有 43 例(4.5%)患者在 ED 就诊后 30 天内死亡。suPAR≥6ng/ml 与死亡率升高相关:qSOFA=0 时为 5.5%比 0.9%(P<0.01),qSOFA≥1 时为 10.7%比 2.1%(P=0.02)。降钙素原≥0.25ng/ml 与死亡率也相关:qSOFA=0 时为 5.5%比 1.9%(P=0.02),qSOFA≥1 时为 11.9%比 4.1%(P=0.03)。在 NEWS<7 的患者中也发现了类似的关联(suPAR 为 5.9%比 1.2%,降钙素原为 7.0%比 1.7%,P<0.001)。
在这项前瞻性队列研究中,suPAR 和降钙素原与 qSOFA 低值或高值以及 NEWS2 低值患者的死亡率升高相关。