Department of Nephrology and Organ Transplantation, Atılım University School of Medicine, Medicana International Ankara Hospital, Ankara, Turkey.
Department of Nephrology and Organ Transplantation, Yeni Yuzyil University Private Gaziosmanpaşa Hospital, Istanbul, Turkey.
Int Urol Nephrol. 2023 Nov;55(11):2989-2999. doi: 10.1007/s11255-023-03645-7. Epub 2023 Jun 8.
Sodium-glucose co-transporter-2 inhibitor (SGLT-2i) administration is associated with some concerns in regard to the increased risk of genital and urinary tract infections (UTI) in kidney transplant recipients (KTR). In this study, we present the results of SGLT-2i use in KTR, including the early post-transplant period.
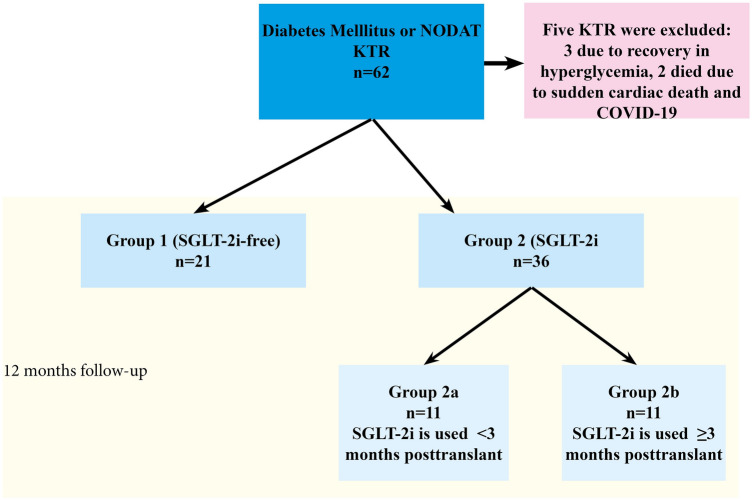
Participants were divided into two groups: SGLT-2i-free diabetic KTR (Group 1, n = 21) and diabetic KTR using SGLT-2i (Group 2, n = 36). Group 2 was further divided into two subgroups according to the posttransplant prescription day of SGLT-2i; < 3 months (Group 2a) and ≥ 3 months (Group 2b). Groups were compared for development of genital and urinary tract infections, glycated hemoglobin a1c (HgbA1c), estimated glomerular filtration rate (eGFR), proteinuria, weight change, and acute rejection rate during 12-month follow-up.
Urinary tract infections prevalence was 21.1% and UTI-related hospitalization rate was 10.5% in our cohort. Prevalence of UTI and UTI-related hospitalization, eGFR, HgbA1c levels, and weight gain were similar between the SGLT-2i group and SGLT-2i-free group, at the 12-month follow-up. UTI prevalence was similar between groups 2a and 2b (p = 0.871). No case of genital infection was recorded. Significant proteinuria reduction was observed in Group 2 (p = 0.008). Acute rejection rate was higher in the SGLT-2i-free group (p = 0.040) and had an impact on 12-month follow-up eGFR (p = 0.003).
SGLT-2i in KTR is not associated with an increased risk of genital infection and UTI in diabetic KTR, even in the early posttransplant period. The use of SGLT-2i reduces proteinuria in KTR and has no adverse effects on allograft function at the 12-month follow-up.
钠-葡萄糖协同转运蛋白 2 抑制剂(SGLT-2i)的应用与肾移植受者(KTR)生殖道和尿路感染(UTI)风险增加有关。本研究报告了 SGLT-2i 在 KTR 中的应用结果,包括移植后早期。
参与者分为两组:无 SGLT-2i 的糖尿病 KTR(组 1,n=21)和使用 SGLT-2i 的糖尿病 KTR(组 2,n=36)。根据 SGLT-2i 移植后处方天数将组 2 进一步分为两个亚组;<3 个月(组 2a)和≥3 个月(组 2b)。比较两组在 12 个月随访期间发生生殖道和尿路感染、糖化血红蛋白 A1c(HgbA1c)、估算肾小球滤过率(eGFR)、蛋白尿、体重变化和急性排斥反应的发生率。
本队列中尿路感染的患病率为 21.1%,UTI 相关住院率为 10.5%。在 12 个月随访时,SGLT-2i 组和 SGLT-2i 组之间的 UTI 患病率、UTI 相关住院率、eGFR 水平、HgbA1c 水平和体重增加相似。组 2a 和组 2b 之间的 UTI 患病率相似(p=0.871)。未记录到生殖器感染病例。组 2 中蛋白尿显著减少(p=0.008)。无 SGLT-2i 组的急性排斥反应发生率较高(p=0.040),并对 12 个月随访时的 eGFR 有影响(p=0.003)。
SGLT-2i 在 KTR 中应用与糖尿病 KTR 中生殖器感染和 UTI 风险增加无关,即使在移植后早期也是如此。SGLT-2i 的使用可减少 KTR 的蛋白尿,并且在 12 个月随访时对移植物功能没有不良影响。