Department of Internal Medicine, University of Pittsburgh Medical Center (UPMC), Pittsburgh, PA, USA.
Department of Internal Medicine, University of Oklahoma Health Sciences Center, Oklahoma City, OK, USA.
ESC Heart Fail. 2023 Aug;10(4):2534-2540. doi: 10.1002/ehf2.14430. Epub 2023 Jun 9.
In this study, we estimated the 30 day all-cause and heart failure-specific readmission rates, predictors, mortality, and hospitalization costs in patients with obstructive sleep apnoea admitted with acute decompensated heart failure with reduced ejection fraction.
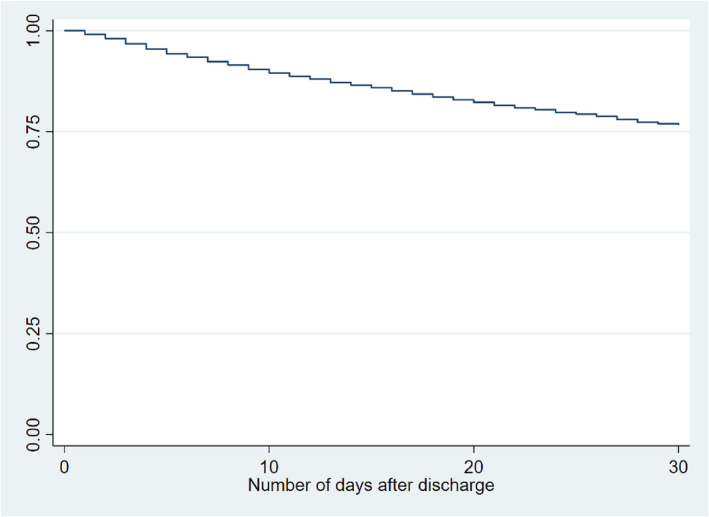
This is a retrospective cohort study using the Agency of Healthcare Research and Quality's National Readmission Database for the year 2019. The primary outcome was the 30 day all-cause hospital readmission rate. The secondary outcomes were (i) in-hospital mortality rate for index admissions; (ii) 30 day mortality rate for index hospitalizations; (iii) the five most common principal diagnosis for readmission; (iv) readmission in-hospital mortality rate; (v) length of hospital stay; (vi) independent risk factors for readmission; and (vii) hospitalization costs. We identified 6908 hospitalizations that met our study definition. The mean patient age was 62.8 years, and women comprised only 27.6% of patients. The 30 day all-cause readmission rate was 23.4%. 48.9% of readmissions were due to decompensated heart failure. The in-hospital mortality rate during readmissions was significantly higher than that of the index admission (5.6% vs. 2.4%; P < 0.05). The mean length of stay for patients during index admissions was 6.5 days (6.06-7.02), while during readmissions, it was 8.5 days (7.4-9.6; P < 0.05). The mean total hospitalization charges at index admissions were $78 438 (68 053-88 824), while during readmissions, they were higher at $124 282 (90 906-157 659; P < 0.05). The mean total cost of hospitalization during index admissions was $20 535 (18 311-22 758), while at readmissions, it was higher at $29 954 (24 041-35 867; P < 0.05). The total hospital charges for all 30 day readmissions were $195 million, and total hospital costs was $46.9 million. The variables found to be associated with increased rate of readmissions were patients with Medicaid insurance, higher Charlson co-morbidity Index, and longer length of stay. The variables associated with lower rate of readmissions were prior percutaneous coronary intervention and patients with private insurance.
In patients with obstructive sleep apnoea admitted with heart failure with reduced ejection fraction, we found a substantial all-cause readmission rate of 23.4% with heart failure readmission constituting about 48.9% of readmissions. Readmissions were associated with higher mortality and resource use.
本研究旨在评估射血分数降低的急性失代偿性心力衰竭合并阻塞性睡眠呼吸暂停患者 30 天全因和心力衰竭特异性再入院率、预测因素、死亡率和住院费用。
这是一项使用 2019 年美国医疗保健研究与质量局国家再入院数据库的回顾性队列研究。主要结局为 30 天全因医院再入院率。次要结局包括:(i)指数入院的院内死亡率;(ii)指数住院的 30 天死亡率;(iii)再入院的前 5 种最常见主要诊断;(iv)再入院院内死亡率;(v)住院时间;(vi)再入院的独立危险因素;以及(vii)住院费用。我们确定了符合研究定义的 6908 例住院患者。患者平均年龄为 62.8 岁,女性仅占患者的 27.6%。30 天全因再入院率为 23.4%。48.9%的再入院是由于心力衰竭失代偿。再入院的院内死亡率明显高于指数入院(5.6%比 2.4%;P<0.05)。指数入院期间患者的平均住院时间为 6.5 天(6.06-7.02),而再入院期间为 8.5 天(7.4-9.6;P<0.05)。指数入院的总住院费用为 78438 美元(68053-88824),而再入院的费用更高,为 124282 美元(90906-157659;P<0.05)。指数入院的总住院费用为 20535 美元(18311-22758),而再入院的费用更高,为 29954 美元(24041-35867;P<0.05)。所有 30 天再入院的总住院费用为 1.95 亿美元,总住院费用为 4690 万美元。与再入院率增加相关的变量包括:接受医疗补助保险的患者、较高的 Charlson 合并症指数和较长的住院时间。与再入院率降低相关的变量包括:先前经皮冠状动脉介入治疗和私人保险患者。
在因射血分数降低的心力衰竭合并阻塞性睡眠呼吸暂停而入院的患者中,我们发现全因再入院率高达 23.4%,心力衰竭再入院占再入院的 48.9%。再入院与更高的死亡率和资源利用相关。