Department of Urology, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, 310016, Zhejiang, China.
World J Surg Oncol. 2023 Jun 12;21(1):179. doi: 10.1186/s12957-023-03049-y.
The occurrence of postoperative complications was associated with poor outcomes for patients undergoing robotic-assisted radical prostatectomy. A prediction model with easily accessible indices could provide valuable information for surgeons. This study aims to identify novel predictive circulating biomarkers significantly associated with surgical complications.
We consecutively assessed all multiport robotic-assisted radical prostatectomies performed between 2021 and 2022. The clinicopathological factors and perioperative levels of multiple circulating markers were retrospectively obtained from the included patients. The associations of these indices with Clavien-Dindo grade II or greater complications, and surgical site infection were assessed using univariable and multivariable logistic regression models. Further, the models were validated for the overall performance, discrimination, and calibration.
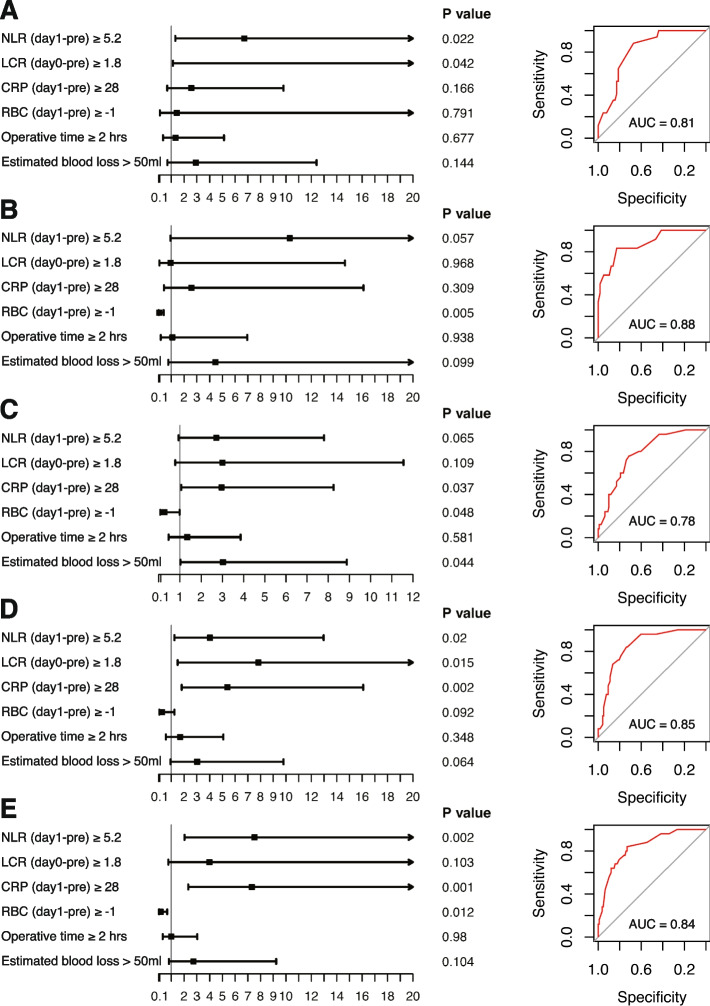
In total, 229 patients with prostate cancer were enrolled in this study. Prolonged operative time could independently predict surgical site infection (OR, 3.39; 95% CI, 1.09-10.54). Higher RBC (day 1-pre) implied lower risks of grade II or greater complications (OR, 0.24; 95% CI, 0.07-0.76) and surgical site infection (OR, 0.23; 95% CI, 0.07-0.78). Additionally, RBC (day 1-pre) independently predicted grade II or greater complications of obese patients (P value = 0.005) as well as those in higher NCCN risk groups (P value = 0.012). Regarding the inflammatory markers, NLR (day 1-pre) (OR, 3.56; 95% CI, 1.37-9.21) and CRP (day 1-pre) (OR, 4.16; 95% CI, 1.69-10.23) were significantly associated with the risk of grade II or greater complications, and both the indices were independent predictors in those with higher Gleason score, or in higher NCCN risk groups (P value < 0.05). The NLR (day 0-pre) could also predict the occurrence of surgical site infection (OR, 5.04; 95% CI, 1.07-23.74).
The study successfully identified novel circulating markers to assess the risk of surgical complications. Postoperative increase of NLR and CRP were independent predictors for grade II or greater complications, especially in those with higher Gleason score, or in higher NCCN risk groups. Additionally, a marked decrease of RBC after the surgery also indicated a higher possibility of surgical complications, especially for the relatively difficult procedures.
术后并发症的发生与接受机器人辅助根治性前列腺切除术的患者预后不良有关。具有易于获取的指标的预测模型可为外科医生提供有价值的信息。本研究旨在确定与手术并发症显著相关的新型预测性循环生物标志物。
我们连续评估了 2021 年至 2022 年间进行的所有多端口机器人辅助根治性前列腺切除术。回顾性地从纳入的患者中获得了临床病理因素和围手术期多个循环标志物的水平。使用单变量和多变量逻辑回归模型评估这些指标与 Clavien-Dindo 分级 II 或更高的并发症和手术部位感染的关联。此外,还对模型的整体性能、区分度和校准进行了验证。
本研究共纳入 229 例前列腺癌患者。手术时间延长可独立预测手术部位感染(OR,3.39;95%CI,1.09-10.54)。较高的 RBC(术前第 1 天)提示 II 级或更高级别并发症(OR,0.24;95%CI,0.07-0.76)和手术部位感染(OR,0.23;95%CI,0.07-0.78)的风险较低。此外,RBC(术前第 1 天)还可以独立预测肥胖患者(P 值=0.005)和 NCCN 风险较高组(P 值=0.012)的 II 级或更高级别并发症。关于炎症标志物,NLR(术前第 1 天)(OR,3.56;95%CI,1.37-9.21)和 CRP(术前第 1 天)(OR,4.16;95%CI,1.69-10.23)与 II 级或更高级别并发症的风险显著相关,这两个指标在 Gleason 评分较高或 NCCN 风险较高的患者中均为独立预测因素(P 值<0.05)。NLR(术前第 0 天)也可以预测手术部位感染的发生(OR,5.04;95%CI,1.07-23.74)。
本研究成功确定了新型循环标志物来评估手术并发症的风险。术后 NLR 和 CRP 的增加是 II 级或更高级别并发症的独立预测因素,尤其是在 Gleason 评分较高或 NCCN 风险较高的患者中。此外,手术后 RBC 的显著下降也表明手术并发症的可能性更高,尤其是对于相对困难的手术。