Department of Urology, Erasmus MC Cancer Institute, Rotterdam, the Netherlands.
Department of Medical Oncology, Erasmus MC Cancer Institute, Rotterdam, the Netherlands.
BMC Cancer. 2023 Jun 13;23(1):539. doi: 10.1186/s12885-023-10963-7.
Patients with locally advanced irresectable or clinically node positive urothelial cancer (UC) have a poor outcome. Currently, these patients can only be cured by receiving induction chemotherapy and, if an adequate radiological response is obtained, radical surgical resection. Long-term survival, however, strongly depends on the absence of residual tumor in the surgical resection specimen, i.e. a pathological complete response (pCR). The reported pCR rate following induction chemotherapy in locally advanced or clinically node-positive UC is 15%. The 5-year overall survival rate for patients achieving a pCR is 70-80% versus 20% for patients who have residual disease or nodal metastases. This clearly demonstrates the unmet need to improve clinical outcome of these patients. Recently, the JAVELIN Bladder 100 study demonstrated an overall survival benefit of sequential chemo-immunotherapy in patients with metastatic UC. The CHASIT study aims to translate these findings to the induction setting by assessing the efficacy and safety of sequential chemo-immunotherapy in patients with locally advanced or clinically node-positive UC. In addition, patient biomaterials are collected to investigate biological mechanisms of response and resistance to chemo-immunotherapy.
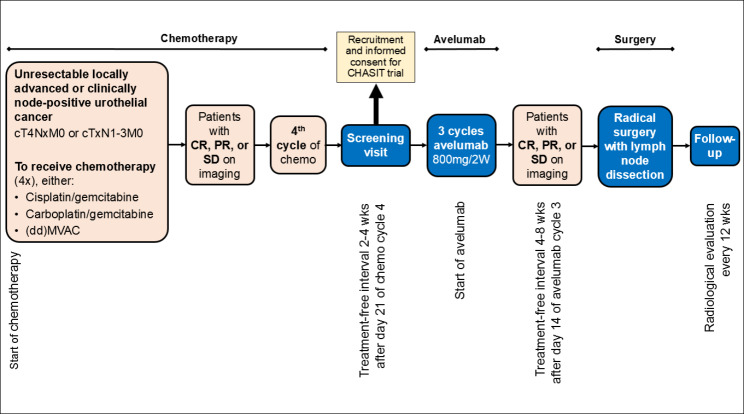
This multicenter, prospective phase II clinical trial includes patients with stage cT4NxM0 or cTxN1-N3M0 UC of the bladder, upper urinary tract or urethra. Patients who do not experience disease progression after 3 or 4 cycles of platinum-based chemotherapy are eligible for inclusion. Included patients receive 3 cycles of anti-PD-1 immunotherapy with avelumab followed by radical surgery. Primary endpoint is the pCR rate. It is hypothesized that sequential chemo-immunotherapy results in a pCR rate of ≥ 30%. To obtain a power of 80%, 64 patients are screened and 58 patients are included in the efficacy analysis. Secondary endpoints are toxicity, postoperative surgical complications, progression-free, cancer-specific and overall survival at 24 months.
This is the first study to assess the potential benefit of sequential chemo-immunotherapy in patients with locally advanced or node positive UC. If the primary endpoint of the CHASIT study is met, i.e. a pCR rate of ≥ 30%, a randomized controlled trial is foreseen to compare this new treatment regimen to standard care.
NCT05600127 at Clinicaltrials gov, registered on 31/10/2022.
局部晚期不可切除或临床淋巴结阳性的尿路上皮癌(UC)患者预后较差。目前,这些患者只能通过接受诱导化疗,如果获得足够的影像学反应,则进行根治性手术切除。然而,长期生存强烈依赖于手术切除标本中无残留肿瘤,即病理完全缓解(pCR)。在局部晚期或临床淋巴结阳性 UC 患者中,诱导化疗后的 pCR 率为 15%。达到 pCR 的患者 5 年总生存率为 70-80%,而有残留疾病或淋巴结转移的患者为 20%。这清楚地表明需要改善这些患者的临床结果。最近,JAVELIN Bladder 100 研究表明,转移性 UC 患者序贯化疗免疫治疗具有总体生存获益。CHASIT 研究旨在通过评估局部晚期或临床淋巴结阳性 UC 患者序贯化疗免疫治疗的疗效和安全性,将这些发现转化为诱导治疗。此外,还收集了患者生物材料,以研究对化疗免疫治疗的反应和耐药的生物学机制。
这是一项多中心、前瞻性的 II 期临床试验,纳入了膀胱、上尿路或尿道的 cT4NxM0 或 cTxN1-N3M0 期 UC 患者。接受铂类为基础的化疗 3 或 4 周期后未发生疾病进展的患者有资格入组。入组患者接受 3 周期抗 PD-1 免疫治疗avelumab,然后进行根治性手术。主要终点是 pCR 率。假设序贯化疗免疫治疗的 pCR 率≥30%。为了获得 80%的效能,筛选了 64 例患者,58 例患者纳入疗效分析。次要终点是毒性、术后手术并发症、无进展、癌症特异性和 24 个月的总生存。
这是第一项评估局部晚期或淋巴结阳性 UC 患者序贯化疗免疫治疗潜在获益的研究。如果 CHASIT 研究的主要终点达到,即 pCR 率≥30%,预计将进行一项随机对照试验,比较这种新的治疗方案与标准治疗。
NCT05600127 在 Clinicaltrials.gov 注册,注册日期为 2022 年 10 月 31 日。