Department of Pharmacy, Research Institute for Medical Innovation, Radboud University Medical Center, Nijmegen, The Netherlands.
Division of Clinical Pharmacology, Department of Medicine, University of Cape Town, South Africa.
Clin Infect Dis. 2023 Sep 18;77(6):875-882. doi: 10.1093/cid/ciad267.
We evaluated the pharmacokinetics of tenofovir alafenamide fumarate (TAF) and tenofovir in a subset of African children enrolled in the CHAPAS-4 trial.
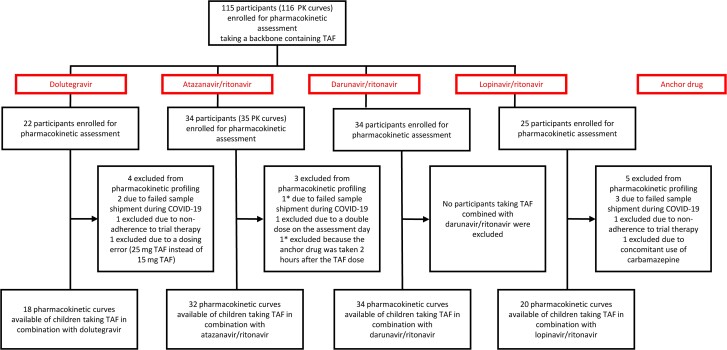
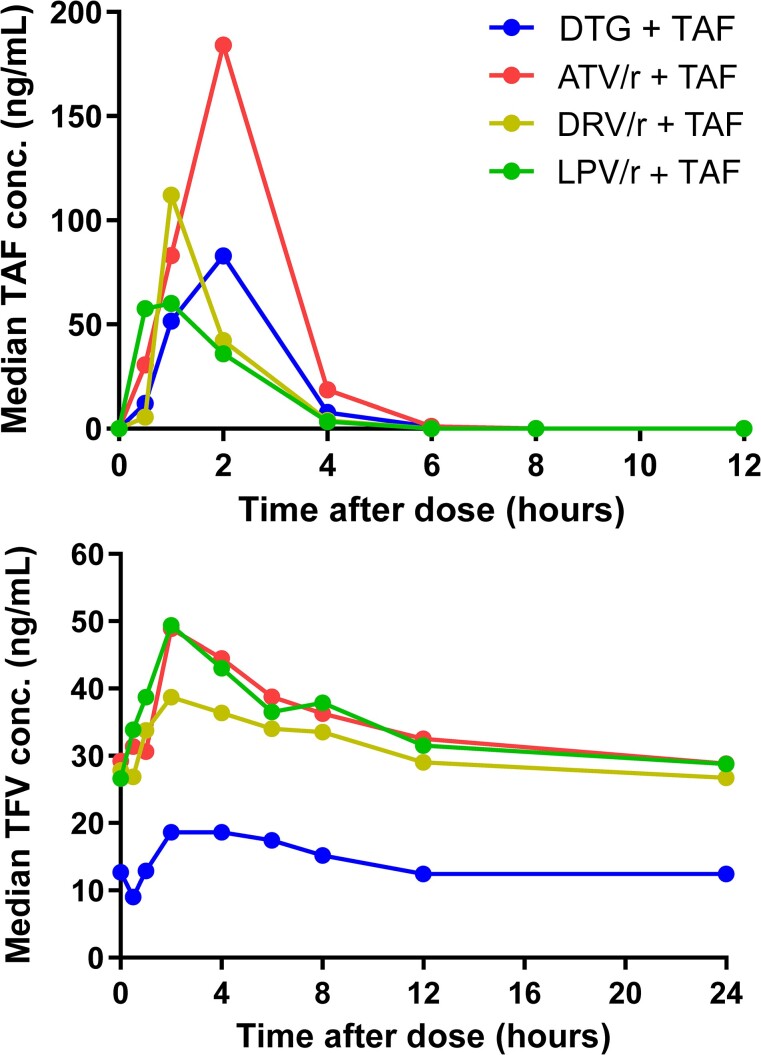
Children aged 3-15 years with human immunodeficiency virus infection failing first-line antiretroviral therapy were randomized to emtricitabine/TAF versus standard-of-care nucleoside reverse transcriptase inhibitor combination, plus dolutegravir, atazanavir/ritonavir, darunavir/ritonavir, or lopinavir/ritonavir. Daily emtricitabine/TAF was dosed according to World Health Organization (WHO)-recommended weight bands: 120/15 mg in children weighing 14 to <25 kg and 200/25 mg in those weighing ≥25 kg. At steady state, 8-9 blood samples were taken to construct pharmacokinetic curves. Geometric mean (GM) area under the concentration-time curve (AUC) and the maximum concentration (Cmax) were calculated for TAF and tenofovir and compared to reference exposures in adults.
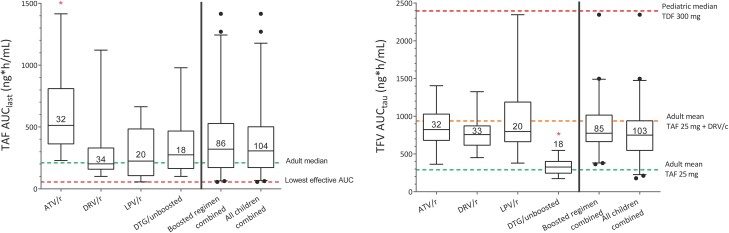
Pharmacokinetic results from 104 children taking TAF were analyzed. GM (coefficient of variation [CV%]) TAF AUClast when combined with dolutegravir (n = 18), darunavir/ritonavir (n = 34), or lopinavir/ritonavir (n = 20) were 284.5 (79), 232.0 (61), and 210.2 (98) nghour/mL, respectively, and were comparable to adult reference values. When combined with atazanavir/ritonavir (n = 32), TAF AUClast increased to 511.4 (68) nghour/mL. For each combination, tenofovir GM (CV%) AUCtau and Cmax remained below reference values in adults taking 25 mg TAF with a boosted protease inhibitors.
In children, TAF combined with boosted PIs or dolutegravir and dosed according to WHO-recommended weight bands provides TAF and tenofovir concentrations previously demonstrated to be well tolerated and effective in adults. These data provide the first evidence for use of these combinations in African children.
ISRCTN22964075.
我们评估了十-酸替诺福韦艾拉酚胺富马酸盐(TAF)和替诺福韦在 CHAPAS-4 试验中入组的一部分非洲儿童中的药代动力学。
感染人类免疫缺陷病毒并正在接受一线抗逆转录病毒治疗的 3-15 岁儿童,随机分为恩曲他滨/TAF 组与标准护理核苷逆转录酶抑制剂联合治疗组,联合药物为多替拉韦、阿扎那韦/利托那韦、达芦那韦/利托那韦或洛匹那韦/利托那韦。每日恩曲他滨/TAF 剂量根据世界卫生组织(WHO)推荐的体重组进行调整:体重 14-<25kg 的儿童使用 120/15mg 剂量,体重≥25kg 的儿童使用 200/25mg 剂量。在稳态时,采集 8-9 个血样以构建药代动力学曲线。计算 TAF 和替诺福韦的几何均数(GM)(变异系数[CV%])下的浓度-时间曲线面积(AUC)和最大浓度(Cmax),并与成人参考值进行比较。
对 104 名服用 TAF 的儿童的药代动力学结果进行了分析。当与多替拉韦(n=18)、达芦那韦/利托那韦(n=34)或洛匹那韦/利托那韦(n=20)联合使用时,TAF 的 GM(CV%)AUClast 分别为 284.5(79)、232.0(61)和 210.2(98)nghour/mL,与成人参考值相当。当与阿扎那韦/利托那韦(n=32)联合使用时,TAF AUClast 增加到 511.4(68)nghour/mL。对于每种联合用药,替诺福韦的 GM(CV%)AUCtau 和 Cmax 仍然低于成人服用 25mg TAF 联合增效蛋白酶抑制剂时的参考值。
在儿童中,TAF 联合增效蛋白酶抑制剂或多替拉韦,并按照 WHO 推荐的体重组进行剂量调整,可提供先前在成人中证明耐受良好且有效的 TAF 和替诺福韦浓度。这些数据为在非洲儿童中使用这些联合用药提供了首个证据。
ISRCTN22964075。