Lim Endry H T, Vlaar Alexander P J, de Bruin Sanne, Rückinger Simon, Thielert Claus, Habel Maria, Guo Renfeng, Burnett Bruce P, Dickinson James, Brouwer Matthijs C, Riedemann Niels C, van de Beek Diederik
Department of Intensive Care Medicine, Amsterdam UMC Location University of Amsterdam, AMC Room C3-421, Meibergdreef 9, 1105 AZ, Amsterdam, The Netherlands.
Department of Neurology, Amsterdam UMC Location University of Amsterdam, Meibergdreef 9, Amsterdam, The Netherlands.
Intensive Care Med Exp. 2023 Jun 19;11(1):37. doi: 10.1186/s40635-023-00520-8.
Vilobelimab, a complement 5a (C5a)-specific monoclonal antibody, reduced mortality in critically ill COVID-19 patients in a phase 3 multicentre, randomized, double-blind, placebo-controlled study. As part of the study, vilobelimab concentrations and C5a levels as well as antidrug antibodies (ADAs) to vilobelimab were analysed.
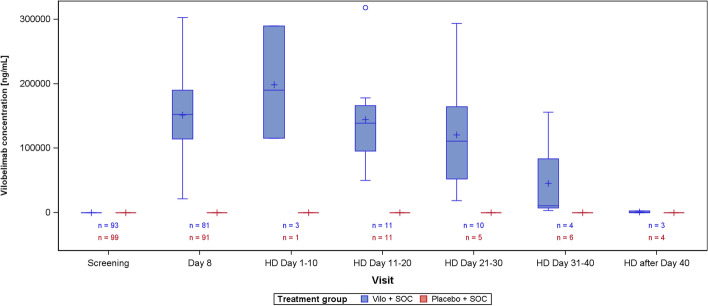
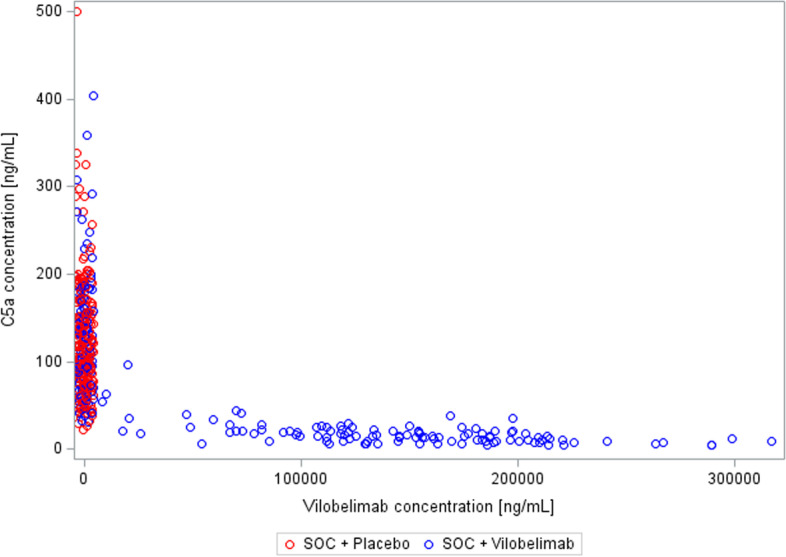
From Oct 1, 2020 to Oct 4, 2021, 368 invasively mechanically ventilated COVID-19 patients were randomized: 177 patients were randomly assigned to receive vilobelimab while 191 patients received placebo. Pharmacokinetic sampling was only performed at sites in Western Europe. Blood samples for vilobelimab measurements were available for 93 of 177 (53%) patients in the vilobelimab group and 99 of 191 (52%) patients in the placebo group. On day 8, after three infusions, mean vilobelimab (trough) concentrations ranged from 21,799.3 to 302,972.1 ng/mL (geometric mean 137,881.3 ng/mL). Blood samples for C5a measurements were available for 94 of 177 (53%) patients in the vilobelimab group and 99 of 191 (52%) patients in the placebo group. At screening, C5a levels were highly elevated and comparable between groups. In the vilobelimab group, median C5a levels were 118.3 ng/mL [IQR 71.2-168.2 ng/mL] and in the placebo group, median C5a levels were 104.6 ng/mL [IQR 77.5-156.6 ng/mL]. By day 8, median C5a levels were reduced by 87% in the vilobelimab group (median 14.5 ng/mL [IQR 9.5-21.0 ng/mL], p < 0.001) versus an 11% increase in the placebo group (median 119.2 ng/mL [IQR 85.9-152.1 ng/mL]). Beyond day 8, though plasma sampling was sparse, C5a levels did not reach screening levels in the vilobelimab group while C5a levels remained elevated in the placebo group. Treatment-emergent ADAs were observed in one patient in the vilobelimab group at hospital discharge on day 40 and in one patient in the placebo group at hospital discharge on day 25.
This analysis shows that vilobelimab efficiently inhibits C5a in critically ill COVID-19 patients. There was no evidence of immunogenicity associated with vilobelimab treatment. Trial registration ClinicalTrials.gov, NCT04333420. Registered 3 April 2020, https://clinicaltrials.gov/ct2/show/NCT04333420.
维洛贝单抗是一种补体5a(C5a)特异性单克隆抗体,在一项3期多中心、随机、双盲、安慰剂对照研究中降低了重症COVID-19患者的死亡率。作为该研究的一部分,对维洛贝单抗浓度、C5a水平以及针对维洛贝单抗的抗药物抗体(ADA)进行了分析。
从2020年10月1日至2021年10月4日,368例接受有创机械通气的COVID-19患者被随机分组:177例患者被随机分配接受维洛贝单抗治疗,191例患者接受安慰剂治疗。药代动力学采样仅在西欧的研究点进行。维洛贝单抗组177例患者中有93例(53%)、安慰剂组191例患者中有99例(52%)有可用于测量维洛贝单抗的血样。在第8天,经过三次输注后,维洛贝单抗(谷值)平均浓度范围为21,799.3至302,972.1 ng/mL(几何平均值137,881.3 ng/mL)。维洛贝单抗组177例患者中有94例(53%)、安慰剂组191例患者中有99例(52%)有可用于测量C5a的血样。在筛查时,C5a水平高度升高且两组之间相当。维洛贝单抗组C5a水平中位数为118.3 ng/mL[四分位间距71.2 - 168.2 ng/mL],安慰剂组C5a水平中位数为104.6 ng/mL[四分位间距77.5 - 156.6 ng/mL]。到第8天,维洛贝单抗组C5a水平中位数降低了87%(中位数14.5 ng/mL[四分位间距9.5 - 21.0 ng/mL],p < 0.001),而安慰剂组升高了11%(中位数119.2 ng/mL[四分位间距85.9 - 152.1 ng/mL])。在第8天之后,尽管血浆采样较少,但维洛贝单抗组C5a水平未达到筛查水平,而安慰剂组C5a水平仍保持升高。在维洛贝单抗组,1例患者在第40天出院时出现治疗中出现的ADA,在安慰剂组,1例患者在第25天出院时出现治疗中出现的ADA。
该分析表明维洛贝单抗可有效抑制重症COVID-19患者的C5a。没有证据表明维洛贝单抗治疗存在免疫原性。试验注册ClinicalTrials.gov,NCT04333420。于2020年4月3日注册,https://clinicaltrials.gov/ct2/show/NCT04333420。