Department of Anesthesiology, University of Michigan, Ann Arbor, MI.
Michigan Opioid Prescribing Engagement Network, Ann Arbor, MI.
Ann Surg. 2023 Dec 1;278(6):e1185-e1191. doi: 10.1097/SLA.0000000000005937. Epub 2023 Jun 19.
To assess whether the risk of persistent opioid use after surgery varies by payer type.
Persistent opioid use is associated with increased health care utilization and risk of opioid use disorder, opioid overdose, and mortality. Most research assessing the risk of persistent opioid use has focused on privately insured patients. Whether this risk varies by payer type is poorly understood.
This cross-sectional analysis of the Michigan Surgical Quality Collaborative database examined adults aged 18 to 64 years undergoing surgical procedures across 70 hospitals between January 1, 2017 and October 31, 2019. The primary outcome was persistent opioid use, defined a priori as 1+ opioid prescription fulfillment at (1) an additional opioid prescription fulfillment after an initial postoperative fulfillment in the perioperative period or at least 1 fulfillment in the 4 to 90 days after discharge and (2) at least 1 opioid prescription fulfillment in the 91 to 180 days after discharge. The association between this outcome and payer type was evaluated using logistic regression, adjusting for patient and procedure characteristics.
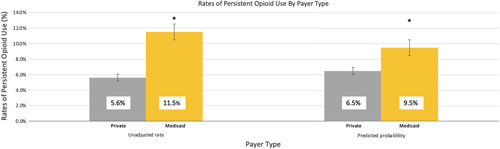
Among 40,071 patients included, the mean age was 45.3 years (SD 12.3), 24,853 (62%) were female, 9430 (23.5%) were Medicaid-insured, 26,760 (66.8%) were privately insured, and 3889 (9.7%) were covered by other payer types. The rate of POU was 11.5% and 5.6% for Medicaid-insured and privately insured patients, respectively (average marginal effect for Medicaid: 2.9% (95% CI 2.3%-3.6%)).
Persistent opioid use remains common among individuals undergoing surgery and higher among patients with Medicaid insurance. Strategies to optimize postoperative recovery should focus on adequate pain management for all patients and consider tailored pathways for those at risk.
评估手术患者的持续性阿片类药物使用风险是否因支付类型而异。
持续性阿片类药物使用与增加医疗保健利用和阿片类药物使用障碍、阿片类药物过量和死亡的风险相关。大多数评估持续性阿片类药物使用风险的研究都集中在私人保险患者上。这种风险是否因支付类型而异尚不清楚。
本项密歇根手术质量协作数据库的横断面分析纳入了 2017 年 1 月 1 日至 2019 年 10 月 31 日期间在 70 家医院接受手术的 18 至 64 岁成年人。主要结局是持续性阿片类药物使用,定义为(1)在围手术期内初始术后获得的阿片类药物处方首次满足后,至少在出院后 4 至 90 天内获得 1 次满足,或(2)在出院后 91 至 180 天内至少获得 1 次满足。使用逻辑回归评估该结局与支付类型之间的关系,同时调整患者和手术特征。
在纳入的 40071 名患者中,平均年龄为 45.3 岁(标准差 12.3),24853 名(62%)为女性,9430 名(23.5%)为医疗补助保险,26760 名(66.8%)为私人保险,3889 名(9.7%)为其他支付类型。POU 发生率分别为医疗补助保险患者的 11.5%和私人保险患者的 5.6%(医疗补助保险的平均边际效应:2.9%(95%CI 2.3%-3.6%))。
手术患者中持续性阿片类药物使用仍然很常见,而医疗补助保险患者的这一比例更高。优化术后康复的策略应重点关注所有患者的充分疼痛管理,并考虑针对那些有风险的患者制定个性化途径。