Division of Pulmonary, Critical Care and Sleep Medicine, Department of Medicine, University of Washington, Seattle, WA, USA.
Department of Biostatistics, Vanderbilt University Medical Center, Nashville, TN, USA.
EBioMedicine. 2023 Jul;93:104667. doi: 10.1016/j.ebiom.2023.104667. Epub 2023 Jun 17.
Severe COVID-19 is associated with innate immunopathology, and CD14, a proximal activator of innate immunity, has been suggested as a potential therapeutic target.
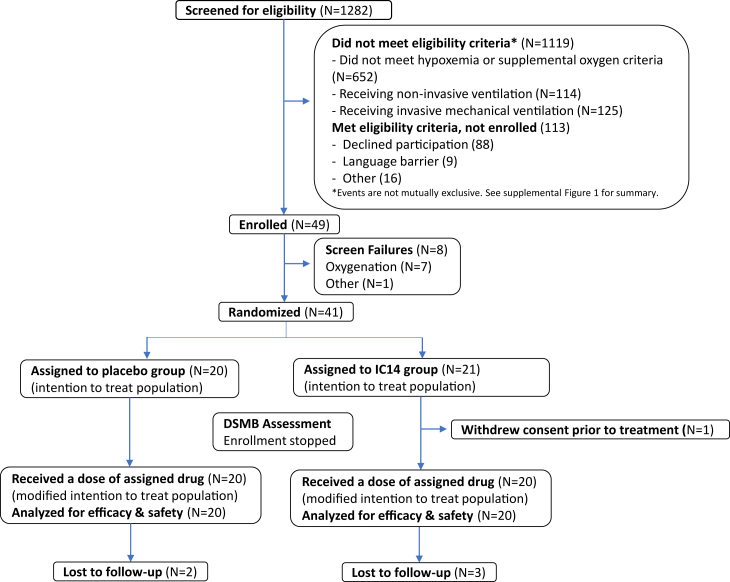
We conducted the COVID-19 anti-CD14 Treatment Trial (CaTT), a Phase II randomized, double-blind, placebo-controlled trial at 5 US-sites between April 12, 2021 and November 30, 2021 (NCT04391309). Hospitalized adults with COVID-19 requiring supplemental oxygen (<30 LPM) were randomized 1:1 to receive 4 daily doses of intravenous IC14, an anti-CD14 monoclonal antibody, or placebo. All participants received remdesivir. The primary outcome was time-to-resolution of illness, defined as improvement on the 8-point NIH-Ordinal COVID-19 Scale to category ≤3. Secondary endpoints were safety and exploratory endpoints were pro-inflammatory and antiviral mediators in serum on days 0-5 & 7. The trial was stopped after 40 patients were randomized and treated due to slow enrollment.
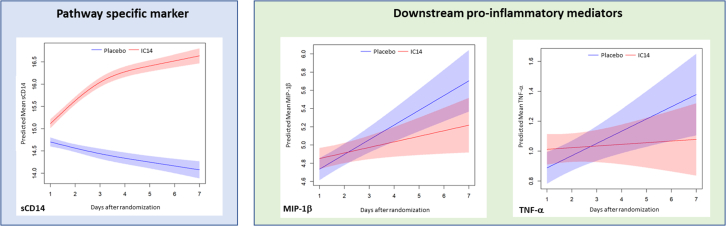
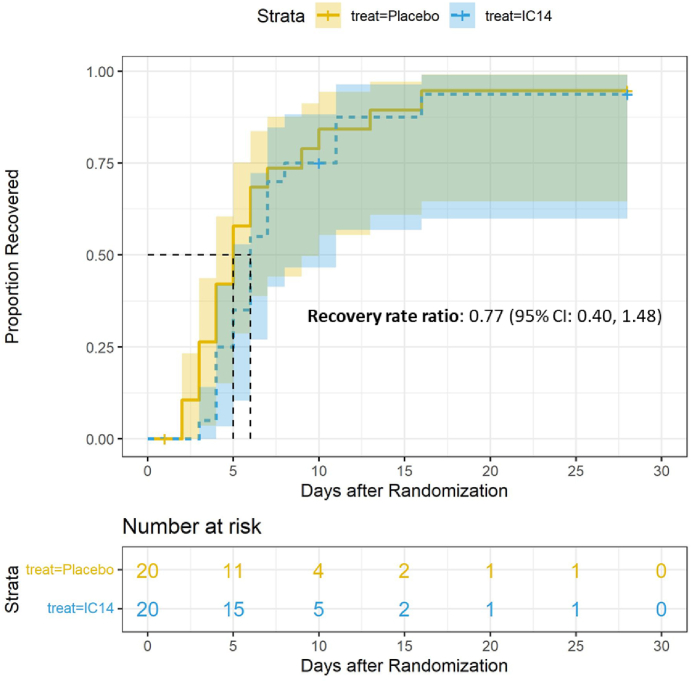
40 participants were randomized and treated with IC14 (n = 20) or placebo (n = 20). The median time-to-recovery was 6 days (95% CI, 5-11) in the IC14 group vs. 5 days (95% CI, 4-10) in the Placebo group (recovery rate ratio: 0.77 (95% CI, 0.40, 1.48) (log-rank p = 0.435). The number of adverse events was similar in each group, and no IC14-attributable secondary infections occurred. In repeated-measures mixed-effects analyses, IC14 treatment increased serum sCD14 concentrations, an expected pharmacodynamic effect. Pre-planned, exploratory analyses suggested that IC14 treatment decreased the trajectories of circulating MIP-1β and TNF-α.
IC14 treatment did not improve time-to-resolution of illness in hypoxemic patients with COVID-19 in this small trial. Results of exploratory analyses suggested IC14 had biologic effects that warrant future clinical investigation.
National Institute of Allergy and Infectious Diseases.
严重的 COVID-19 与先天免疫病理学有关,CD14 作为先天免疫的近端激活物,已被认为是潜在的治疗靶点。
我们在美国 5 个地点进行了 COVID-19 抗 CD14 治疗试验(CaTT),这是一项 2021 年 4 月 12 日至 2021 年 11 月 30 日进行的 II 期随机、双盲、安慰剂对照试验(NCT04391309)。需要补充氧气(<30 LPM)的住院 COVID-19 成人患者按 1:1 随机接受 4 天的静脉注射 IC14(一种抗 CD14 单克隆抗体)或安慰剂。所有参与者均接受瑞德西韦治疗。主要结局是疾病缓解时间,定义为 NIH 序贯 COVID-19 量表评分改善至≤3 分。次要终点是安全性和探索性终点,包括第 0-5 天和第 7 天血清中的促炎和抗病毒介质。由于入组缓慢,在随机分组和治疗 40 例患者后,试验停止。
40 名患者被随机分为 IC14 组(n=20)或安慰剂组(n=20)。IC14 组的中位恢复时间为 6 天(95%CI,5-11),安慰剂组为 5 天(95%CI,4-10)(恢复率比:0.77(95%CI,0.40,1.48)(对数秩检验,p=0.435)。两组的不良事件数量相似,且未发生与 IC14 相关的继发感染。在重复测量混合效应分析中,IC14 治疗增加了血清 sCD14 浓度,这是一种预期的药效学效应。预先计划的探索性分析表明,IC14 治疗降低了循环 MIP-1β 和 TNF-α 的轨迹。
在这项小型试验中,IC14 治疗并未改善低氧血症 COVID-19 患者的疾病缓解时间。探索性分析的结果表明,IC14 具有生物学效应,值得进一步临床研究。
美国国立过敏和传染病研究所。