Cox Daniel R A, McClure Tess, Zhang Fan, Wong Boris Ka Leong, Testro Adam, Goh Su Kah, Muralidharan Vijayaragavan, Dobrovic Alexander
Department of Surgery (Austin Precinct), University of Melbourne, Melbourne, VIC 3084, Australia.
HPB & Liver Transplant Surgery Unit, Department of Surgery, Austin Health, Melbourne, VIC 3084, Australia.
Epigenomes. 2023 Jun 9;7(2):11. doi: 10.3390/epigenomes7020011.
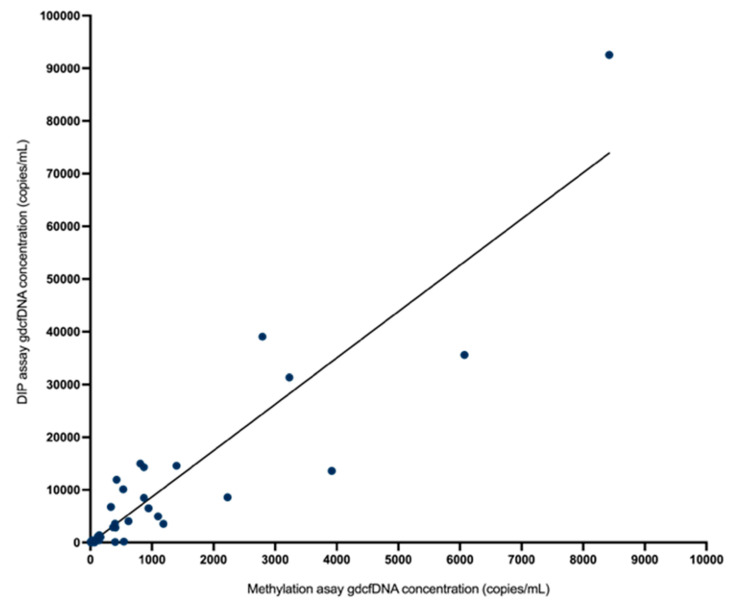
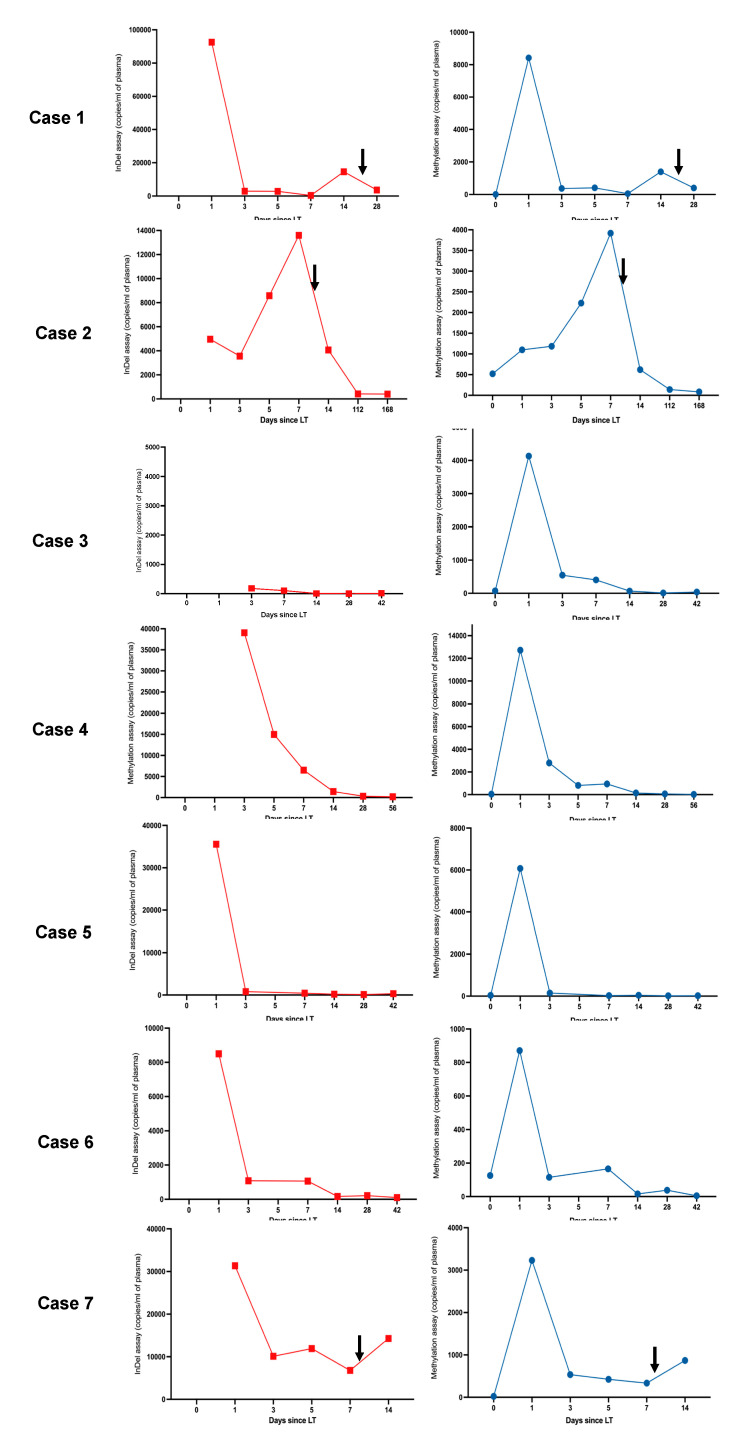
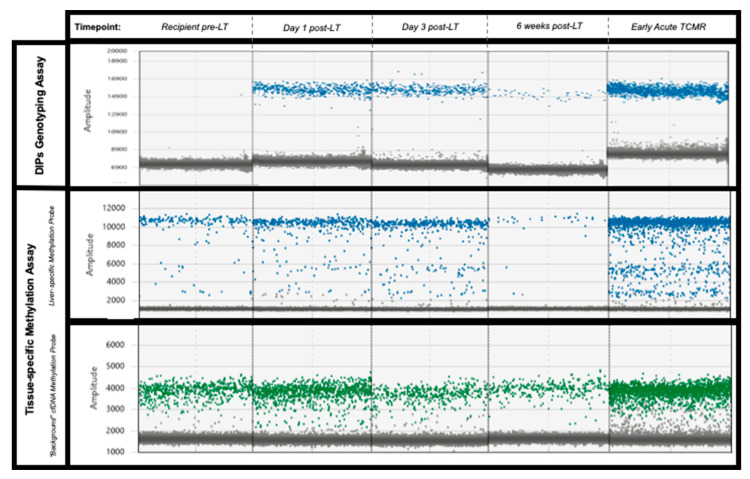
: Graft-derived cell-free DNA (gdcfDNA) analysis has shown promise as a non-invasive tool for monitoring organ health following solid organ transplantation. A number of gdcfDNA analysis techniques have been described; however, the majority rely on sequencing or prior genotyping to detect donor-recipient mis-matched genetic polymorphisms. Differentially methylated regions of DNA can be used to identify the tissue-of-origin of cell-free DNA (cfDNA) fragments. In this study, we aimed to directly compare the performance of gdcfDNA monitoring using graft-specific DNA methylation analysis and donor-recipient genotyping techniques in a pilot cohort of clinical samples from patients post-liver transplantation. : 7 patients were recruited prior to LT, 3 developed early, biopsy-proven TCMR in the first 6 weeks post-LT. gdcfDNA was successfully quantified in all samples using both approaches. There was a high level of technical correlation between results using the two techniques (Spearman testing, r = 0.87, < 0.0001). gdcfDNA levels quantified using the genotyping approach were significantly greater across all timepoints in comparison to the tissue-specific DNA methylation-based approach: e.g., day 1 post-LT median 31,350 copies/mL (IQR 6731-64,058) vs. 4133 copies/mL (IQR 1100-8422), respectively. Qualitative trends in gdcfDNA levels for each patient were concordant between the two assays. Acute TCMR was preceded by significant elevations in gdcfDNA as quantified by both techniques. Elevations in gdcfDNA, using both techniques, were suggestive of TCMR in this pilot study with a 6- and 3-day lead-time prior to histological diagnosis in patients 1 and 2. : Both the graft-specific methylation and genotyping techniques successfully quantified gdcfDNA in patients post-LT with statistically significant concordance. A direct comparison of these two techniques is not only important from a technical perspective for orthogonal validation, but significantly adds weight to the evidence that gdcfDNA monitoring reflects the underlying biology. Both techniques identified LT recipients who developed acute TCMR, with several days lead-time in comparison to conventional diagnostic workflows. Whilst the two assays performed comparably, gdcfDNA monitoring based on graft-specific DNA methylation patterns in cfDNA offers major practical advantages over the donor-recipient genotyping, and hence enhances the potential to translate this emerging technology into clinical practice.
移植物来源的游离DNA(gdcfDNA)分析已显示出有望成为实体器官移植后监测器官健康的非侵入性工具。已经描述了多种gdcfDNA分析技术;然而,大多数技术依赖于测序或先前的基因分型来检测供体-受体错配的遗传多态性。DNA的差异甲基化区域可用于识别游离DNA(cfDNA)片段的组织来源。在本研究中,我们旨在直接比较使用移植物特异性DNA甲基化分析和供体-受体基因分型技术对肝移植术后患者临床样本的试点队列进行gdcfDNA监测的性能。7名患者在肝移植前入组,3名在肝移植术后前6周出现早期经活检证实的急性细胞介导性排斥反应(TCMR)。使用两种方法均成功对所有样本中的gdcfDNA进行了定量。两种技术的结果之间存在高度的技术相关性(Spearman检验,r = 0.87,P < 0.0001)。与基于组织特异性DNA甲基化的方法相比,在所有时间点使用基因分型方法定量的gdcfDNA水平均显著更高:例如,肝移植术后第1天,中位数分别为31,350拷贝/毫升(四分位间距6731 - 64,058)和4133拷贝/毫升(四分位间距1100 - 8422)。两种检测方法中每位患者的gdcfDNA水平的定性趋势一致。两种技术定量的gdcfDNA在急性TCMR之前均显著升高。在本试点研究中,使用两种技术检测到的gdcfDNA升高提示发生了TCMR,在患者1和患者2中,在组织学诊断前分别有6天和3天的提前期。移植物特异性甲基化和基因分型技术均成功对肝移植术后患者的gdcfDNA进行了定量,且具有统计学意义的一致性。这两种技术的直接比较不仅从技术角度对于正交验证很重要,而且显著增加了gdcfDNA监测反映潜在生物学特性的证据的权重。两种技术均识别出发生急性TCMR的肝移植受者,与传统诊断流程相比有几天的提前期。虽然两种检测方法表现相当,但基于cfDNA中移植物特异性DNA甲基化模式的gdcfDNA监测相对于供体-受体基因分型具有主要的实际优势,因此增强了将这项新兴技术转化为临床实践的潜力。