Department of Experimental and Clinical Biomedical Sciences "Mario Serio", University of Florence, Florence, Italy.
Endocrinologic Unit, Azienda Ospedaliera Universitaria Careggi, Florence, Italy.
World J Surg Oncol. 2023 Jun 27;21(1):192. doi: 10.1186/s12957-023-03072-z.
Pheochromocytoma (PHEO) and paraganglioma (PGL) are rare neuroendocrine tumors characterized by hemodynamic instability, caused by the paroxysmal release of catecholamines. Patients may develop cardiovascular complications in the perioperative phase due to the massive release of catecholamines, particularly during anesthetic induction and surgical manipulation of the tumor. The aim of this retrospective study was to evaluate the risk factors involved in perioperative hemodynamic instability in patients who underwent surgery for chromaffin tumors.
Forty patients (median age 55 [36.50-64.50]) undergone surgery for PHEO/abdominal PGL from January 2011 to December 2016 at the AOU Careggi (Florence, Italy) were retrospectively evaluated. Systolic, diastolic, and mean blood pressure were considered at baseline and during surgery. Patients with blood pressure steadily < 140/90 mmHg before surgery were considered "adequately prepared". A preoperative therapy with doxazosin, a selective alpha-1 blocker, was started in all patients for at least 14 days prior to the surgery. The presence of hemodynamic instability was reported.
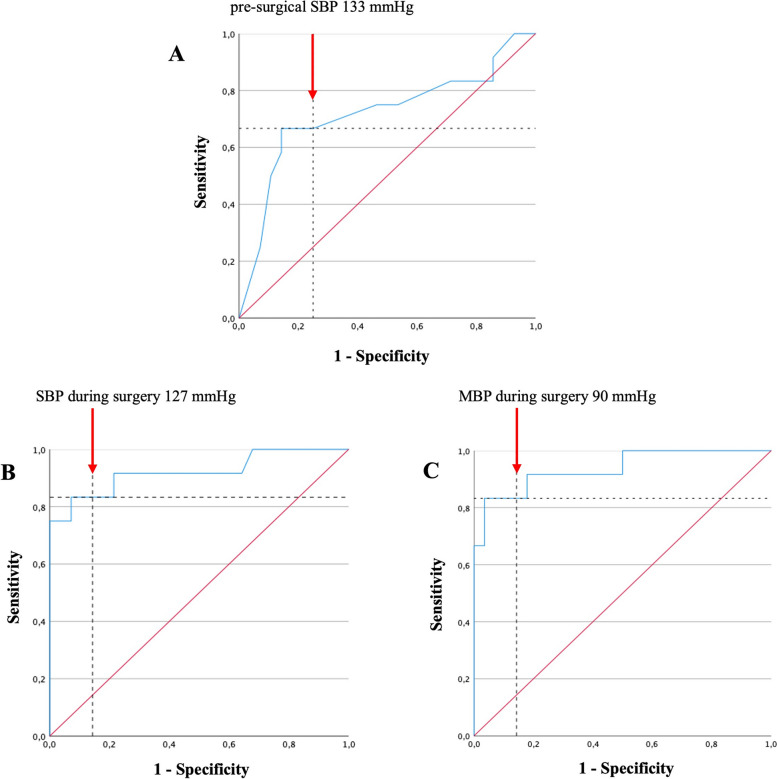
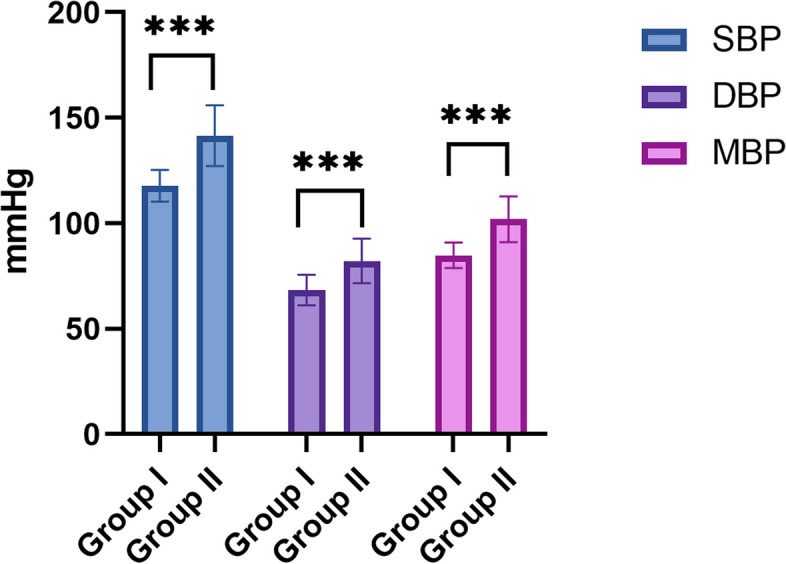
Comparing males and females, a significant difference in doxazosin daily dose (p = 0.018), systolic blood pressure (p = 0.048), and in the proportion of adequately prepared patients (p = 0.031) emerged. A positive correlation between preoperative daily dose of doxazosin, tumor size (B = 0.60, p < 0.001), and urinary normetanephrine levels (B = 0.64, p < 0.001) was also observed. Hemodynamic instability occurred in 30.0% of patients. The absence of adequate preparation (p = 0.012) before surgery, urinary normetanephrine levels (NMNur p = 0.039), and surgery time (minutes) (p = 0.021) resulted as risk factors of hemodynamic instability in our series. The use of intraoperative drugs was higher in patients with hemodynamic instability (p < 0.001). A pre-surgical SBP level of > 133 mmHg (OR = 6 CI95% 1.37-26.20, p = 0.017) and an intraoperative SBP and MBP levels of > 127 mmHg (OR = 28.80 CI95% 2.23-371.0, p = 0.010) and > 90 mmHg (OR = 18.90 CI95% 1.82-196.0, p = 0.014), respectively, were identified as effective thresholds to recognize patients at higher risk of HI.
A preoperative therapy with alpha-blockers is useful, but not sufficient to avoid surgical risks. Patients with higher pre-surgical levels of NMNur, pre-surgical SBP > 133 mmHg, and/or intraoperative SBP > 127 mmHg and MBP > 90 mmHg, should be carefully monitored. A multidisciplinary approach is indispensable to optimize the management of PHEOs/abdominal PGLs in order to reduce surgical complications.
嗜铬细胞瘤(pheochromocytoma,PHEO)和副神经节瘤(paraganglioma,PGL)是罕见的神经内分泌肿瘤,其特征为儿茶酚胺的阵发性释放导致血流动力学不稳定。由于儿茶酚胺的大量释放,患者在围手术期可能会发生心血管并发症,特别是在麻醉诱导和肿瘤手术操作期间。本回顾性研究的目的是评估在因嗜铬细胞瘤而行手术的患者中,围手术期血流动力学不稳定的相关风险因素。
2011 年 1 月至 2016 年 12 月,在意大利佛罗伦萨 AOU 卡尔吉(Careggi)医院对 40 例(中位年龄 55 [36.50-64.50] 岁)因 PHEO/腹部 PGL 而行手术的患者进行了回顾性评估。在基线和手术期间考虑收缩压、舒张压和平均血压。在手术前血压持续稳定<140/90mmHg 的患者被认为是“充分准备”。所有患者在手术前至少 14 天开始接受多沙唑嗪(一种选择性α-1 阻滞剂)术前治疗。报告了血流动力学不稳定的发生情况。
比较男性和女性,多沙唑嗪的日剂量(p=0.018)、收缩压(p=0.048)和充分准备患者的比例(p=0.031)存在显著差异。术前每日多沙唑嗪剂量与肿瘤大小(B=0.60,p<0.001)和尿去甲变肾上腺素水平(B=0.64,p<0.001)呈正相关。在我们的研究中,术前未充分准备(p=0.012)、尿去甲变肾上腺素水平(NMNur p=0.039)和手术时间(分钟)(p=0.021)是血流动力学不稳定的风险因素。在血流动力学不稳定的患者中,术中药物的使用更高(p<0.001)。术前收缩压水平>133mmHg(OR=6,95%CI 1.37-26.20,p=0.017)和术中收缩压和平均动脉压水平>127mmHg(OR=28.80,95%CI 2.23-371.0,p=0.010)和>90mmHg(OR=18.90,95%CI 1.82-196.0,p=0.014)分别被确定为识别高风险 HI 患者的有效阈值。
术前使用α阻滞剂是有用的,但不足以避免手术风险。术前 NMNur 水平较高、术前收缩压>133mmHg 和/或术中收缩压>127mmHg 和平均动脉压>90mmHg 的患者应密切监测。为了降低手术并发症的风险,需要采用多学科方法来优化 PHEOs/腹部 PGL 的管理。