Clavelou Pierre, Castelnovo Giovanni, Pourcher Valérie, De Sèze Jerome, Vermersch Patrick, Ben-Amor Ali-Frederic, Savarin Carine, Defer Gilles
Department of Neurology, Clermont-Ferrand University Hospital, 58 Rue Montalembert, 63003, Clermont-Ferrand Cedex 1, France.
Department of Neurology, Nîmes University Hospital, Hopital Caremeau, Nîmes, France.
Neurol Ther. 2023 Oct;12(5):1457-1476. doi: 10.1007/s40120-023-00496-3. Epub 2023 Jun 29.
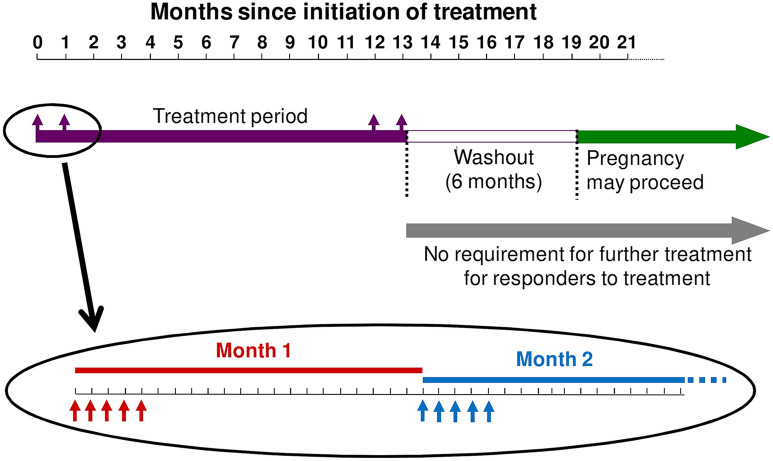
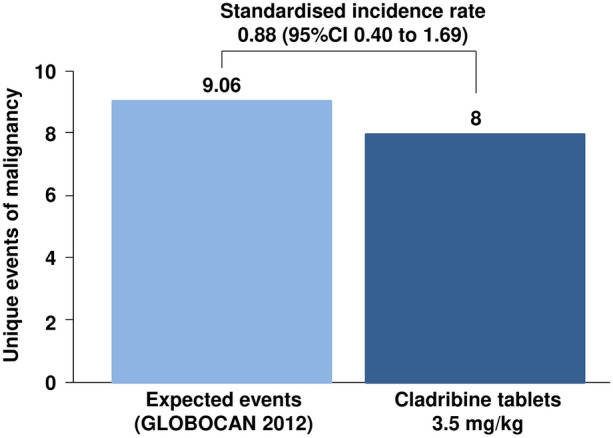
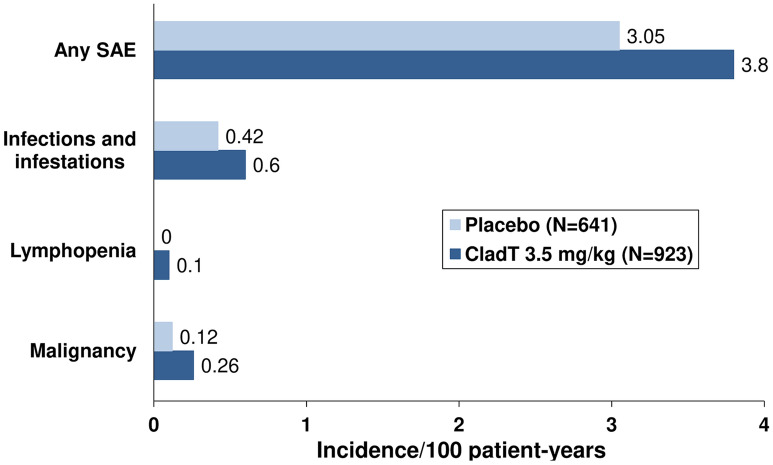
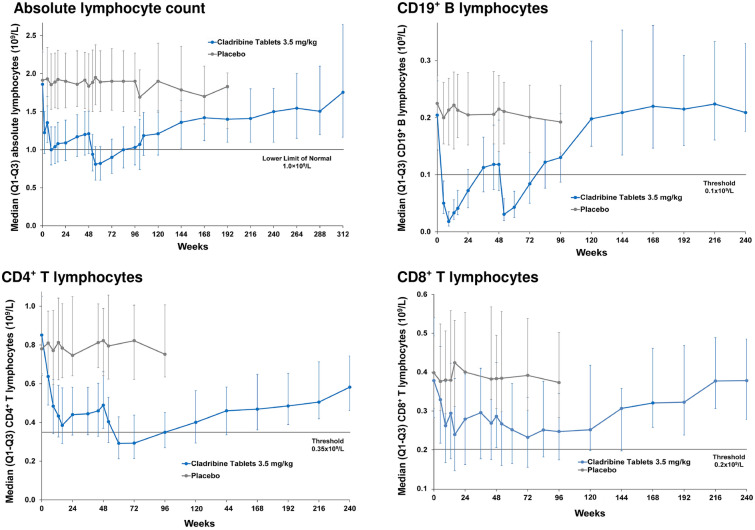
Cladribine tablets (CladT) is a highly active oral disease-modifying therapy (DMT) for the management of relapsing multiple sclerosis (RMS). CladT acts as an immune reconstitution therapy, in that two short courses of treatment 1 year apart have been shown to suppress disease activity for a prolonged period in most patients, without need for continued DMT. Each course of CladT induces a profound reduction in B lymphocytes that recovers over months, and serious lymphopenia (Grade 3-4) is uncommon. Smaller reductions in levels of T lymphocytes occur slightly later: on average, these remain within the normal range and repopulate progressively. A larger effect occurs on CD8 vs. CD4 cells. Reactivation of latent or opportunistic infections (e.g. varicella zoster, tuberculosis) is mostly associated with very low lymphocyte counts (< 200/mm). Screening and managing pre-existing infections, vaccinating non-exposed patients and delaying the 2nd year of treatment with CladT to allow lymphocytes to recover to > 800/mm (if necessary) are important for avoiding infections and higher-grade lymphopenia. There was no demonstrable or apparent effect of CladT on the efficacy of vaccinations, including against Covid-19. Adverse events consistent with drug-induced liver injury (DILI) represent a rare but potentially serious complication of CladT therapy in spontaneous adverse event reporting; patients should be screened for liver dysfunction before starting treatment. Ongoing hepatic monitoring is not required, but CladT must be withdrawn if signs and symptoms of DILI develop. There was a numerical imbalance for malignancies when comparing cladribine to placebo in the clinical programme, particularly in short-term data, but recent evidence shows that the risk of malignancy with CladT is similar to the background rate in the general population and to that with other DMTs. Overall, CladT is well tolerated with a favorable safety profile appropriate for the management of RMS.
克拉屈滨片(CladT)是一种用于治疗复发型多发性硬化症(RMS)的高效口服疾病修正疗法(DMT)。CladT作为一种免疫重建疗法,间隔1年的两个短疗程治疗已被证明可在大多数患者中长时间抑制疾病活动,无需持续使用DMT。CladT的每个疗程都会使B淋巴细胞显著减少,这种减少会在数月内恢复,严重淋巴细胞减少(3-4级)并不常见。T淋巴细胞水平的较小降低出现得稍晚:平均而言,这些仍在正常范围内并逐渐恢复。对CD8细胞的影响比对CD4细胞的影响更大。潜伏性或机会性感染(如水痘带状疱疹、结核病)的重新激活大多与极低的淋巴细胞计数(<200/mm)有关。筛查和管理既往感染、为未接触过感染的患者接种疫苗以及推迟CladT治疗的第二年以使淋巴细胞恢复至>800/mm(如有必要)对于避免感染和更高级别的淋巴细胞减少很重要。CladT对包括针对新冠病毒19的疫苗接种效果没有明显或显著影响。在自发不良事件报告中,与药物性肝损伤(DILI)一致的不良事件是CladT治疗罕见但潜在严重的并发症;患者在开始治疗前应进行肝功能障碍筛查。不需要进行持续的肝脏监测,但如果出现DILI的体征和症状,必须停用CladT。在临床研究中,将克拉屈滨与安慰剂进行比较时,恶性肿瘤存在数值上的不平衡,特别是在短期数据中,但最近的证据表明,CladT导致恶性肿瘤的风险与一般人群的背景发生率以及其他DMT的风险相似。总体而言,CladT耐受性良好,具有适合RMS管理的良好安全性。