Centre for Respiratory Medicine and Allergy, Institute of Inflammation and Repair, Manchester Academic Health Science Centre, University of Manchester, Manchester, UK.
Manchester University NHS Foundation Trust, Manchester, UK.
Adv Ther. 2023 Oct;40(10):4282-4297. doi: 10.1007/s12325-023-02583-1. Epub 2023 Jun 29.
Clinical studies demonstrate an accelerated decline in lung function in patients with moderate chronic obstructive pulmonary disease (COPD) (Global Initiative for Chronic Obstructive Lung Disease [GOLD] grade 2) versus severe and very severe COPD (GOLD grades 3 and 4). This predictive modelling study assessed the impact of initiating pharmacotherapy earlier versus later on long-term disease progression in COPD.
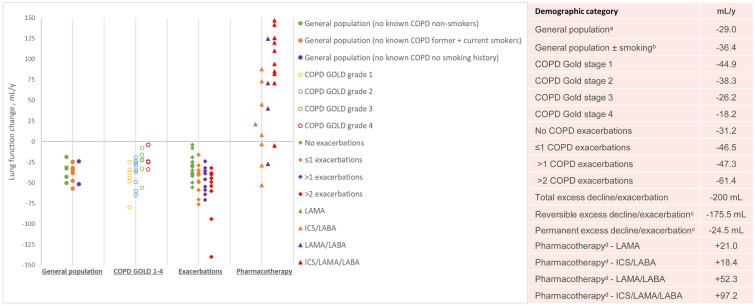
The modelling approach used data on decline in forced expiratory volume in 1 s (FEV) extracted from published studies to develop a longitudinal non-parametric superposition model of lung function decline with progressive impact of exacerbations from 0 per year to 3 per year and no ongoing pharmacotherapy. The model simulated decline in FEV and annual exacerbation rates from age 40 to 75 years in COPD with initiation of long-acting anti-muscarinic antagonist (LAMA)/long-acting beta-agonist (LABA) (umeclidinium (UMEC)/vilanterol (VI)) or triple (inhaled corticosteroid (ICS)/LAMA/LABA; fluticasone furoate (FF)/UMEC/VI) therapy at 40, 55 or 65 years of age.
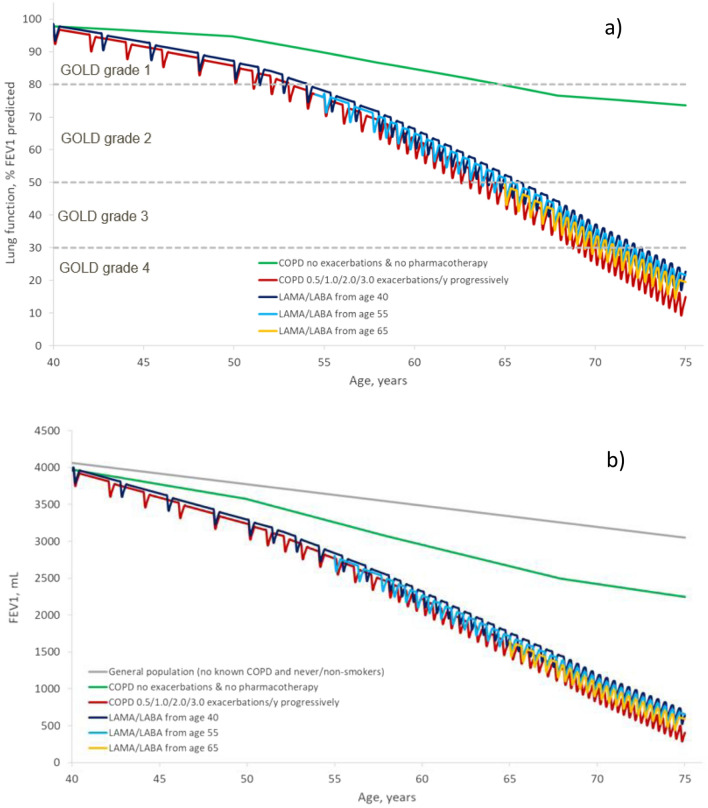
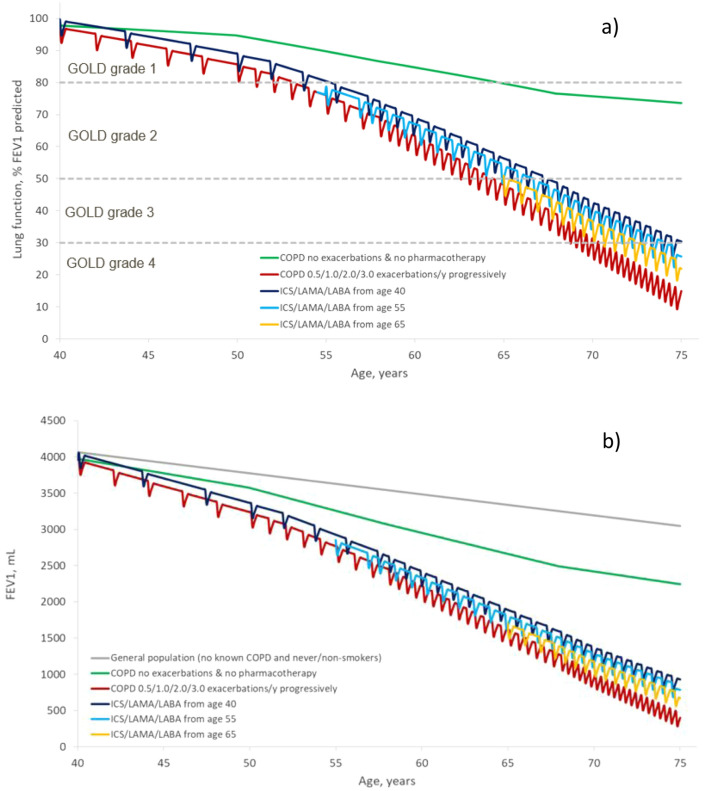
Model-predicted decline in FEV showed that, compared with 'no ongoing' therapy, initiation of triple or LAMA/LABA therapy at age 40, 55 or 65 years preserved an additional 469.7 mL or 236.0 mL, 327.5 mL or 203.3 mL, or 213.5 mL or 137.5 mL of lung function, respectively, by the age of 75. The corresponding average annual exacerbation rates were reduced from 1.57 to 0.91, 1.06 or 1.23 with triple therapy or to 1.2, 1.26 and 1.4 with LAMA/LABA therapy when initiated at 40, 55 or 65 years of age, respectively.
This modelling study suggests that earlier initiation of LAMA/LABA or triple therapy may have positive benefits in slowing disease progression in patients with COPD. Greater benefits were demonstrated with early initiation therapy with triple versus LAMA/LABA.
临床研究表明,与严重和极严重 COPD(GOLD 分级 3 和 4)相比,中度慢性阻塞性肺疾病(COPD)(全球慢性阻塞性肺疾病倡议 [GOLD] 分级 2)患者的肺功能下降速度更快。这项预测模型研究评估了在 COPD 中尽早开始药物治疗与较晚开始药物治疗对长期疾病进展的影响。
该建模方法使用了从已发表的研究中提取的 1 秒用力呼气量(FEV)下降数据,开发了一种与渐进性加重相关的肺功能下降的纵向非参数叠加模型,每年加重 0 次至 3 次,且无持续药物治疗。该模型模拟了从 40 岁到 75 岁 COPD 患者的 FEV 下降和每年加重率,在 40、55 或 65 岁时开始长效抗毒蕈碱拮抗剂(LAMA)/长效β激动剂(LABA)(乌美溴铵(UMEC)/维兰特罗(VI))或三联(吸入皮质类固醇(ICS)/LAMA/LABA;糠酸氟替卡松(FF)/UMEC/VI)治疗。
模型预测的 FEV 下降表明,与“无持续”治疗相比,40、55 或 65 岁时开始三联或 LAMA/LABA 治疗可分别额外保留 469.7mL 或 236.0mL、327.5mL 或 203.3mL 或 213.5mL 或 137.5mL 的肺功能,直至 75 岁。相应的平均每年加重率从 1.57 降至 0.91、1.06 或 1.23,三联治疗或 1.2、1.26 和 1.4,LAMA/LABA 治疗分别在 40、55 或 65 岁时开始治疗。
这项建模研究表明,在 COPD 患者中更早开始 LAMA/LABA 或三联治疗可能对减缓疾病进展有积极益处。与 LAMA/LABA 相比,早期开始三联治疗具有更大的益处。