Department of Medical Imaging, University Health Network, University of Toronto, Toronto, Canada.
Department of Radiology, Concord Repatriation General Hospital, NSW, Concord, NSW, Australia.
Br J Radiol. 2023 Aug;96(1148):20220366. doi: 10.1259/bjr.20220366. Epub 2023 Jun 28.
Quantify the outcomes following pneumothorax aspiration and influence upon chest drain insertion.
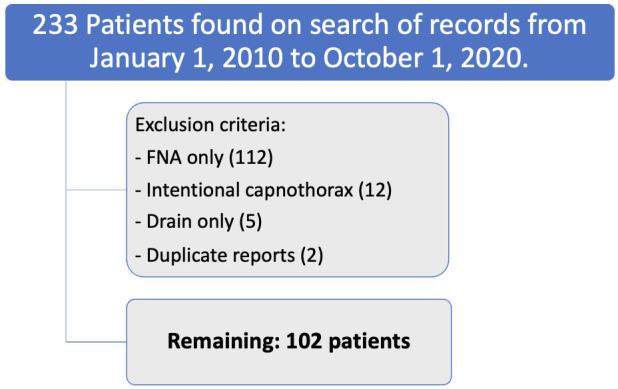
This was a retrospective cohort study of patients who underwent aspiration for the treatment of a pneumothorax following a CT percutaneous transthoracic lung biopsy (CT-PTLB) from January 1, 2010 to October 1, 2020 at a tertiary center. Patient, lesion and procedural factors associated with chest drain insertion were assessed with univariate and multivariate analyses.
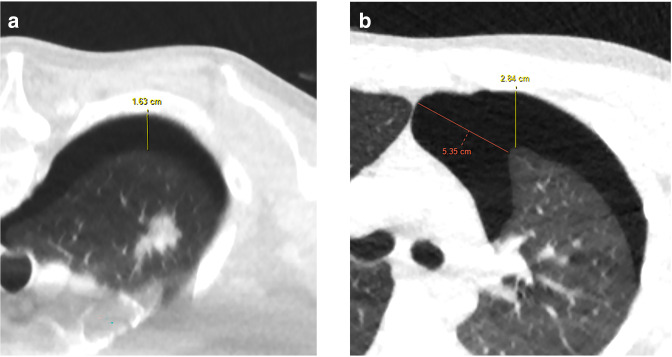
A total of 102 patients underwent aspiration for a pneumothorax following CT-PTLB. Overall, 81 patients (79.4%) had a successful pneumothorax aspiration and were discharged home on the same day. In 21 patients (20.6%), the pneumothorax continued to increase post-aspiration and required chest drain insertion with hospital admission. Significant risk factors requiring chest drain insertion included upper/middle lobe biopsy location [odds ratio (OR) 6.46; 95% CI 1.77-23.65, = 0.003], supine biopsy position (OR 7.06; 95% CI 2.24-22.21, < 0.001), emphysema (OR 3.13; 95% CI 1.10-8.87, = 0.028), greater needle depth ≥2 cm (OR 4.00; 95% CI 1.44-11.07, = 0.005) and a larger pneumothorax (axial depth ≥3 cm) (OR 16.00; 95% CI 4.76-53.83, < 0.001). On multivariate analysis, larger pneumothorax size and supine position during biopsy remained significant for chest drain insertion. Aspiration of a larger pneumothorax (radial depths ≥3 cm and ≥4 cm) had a 50% rate of success. Aspiration of a smaller pneumothorax (radial depth 2-3 cm and <2 cm) had an 82.6% and 100% rate of success, respectively.
Aspiration of pneumothorax after CT-PTLB can help reduce chest drain insertion in approximately 50% of patients with larger pneumothoraces and even more so with smaller pneumothoraces (>80%).
Aspiration of pneumothoraces up to 3 cm was often associated with avoiding chest drain insertion and allowing for earlier discharge.
量化气胸抽气后的结果,并探讨其对胸腔引流管插入的影响。
这是一项回顾性队列研究,纳入了 2010 年 1 月 1 日至 2020 年 10 月 1 日期间在一家三级中心因 CT 经皮肺活检(CT-PTLB)后发生气胸而行抽气治疗的患者。使用单因素和多因素分析评估与胸腔引流管插入相关的患者、病变和操作因素。
共 102 例患者因 CT-PTLB 后发生气胸而行抽气治疗。总体而言,81 例(79.4%)患者气胸抽气成功,并于同日出院。21 例(20.6%)患者气胸在抽气后持续增加,需要胸腔引流管插入和住院治疗。需要胸腔引流管插入的显著危险因素包括上/中叶活检部位(比值比[OR] 6.46;95%可信区间[CI] 1.77-23.65, = 0.003)、仰卧位活检体位(OR 7.06;95%CI 2.24-22.21, < 0.001)、肺气肿(OR 3.13;95%CI 1.10-8.87, = 0.028)、针深度≥2cm(OR 4.00;95%CI 1.44-11.07, = 0.005)和更大的气胸(轴向深度≥3cm)(OR 16.00;95%CI 4.76-53.83, < 0.001)。多因素分析显示,较大的气胸大小和活检时的仰卧位仍是胸腔引流管插入的显著相关因素。抽吸较大的气胸(径向深度≥3cm 和≥4cm)的成功率为 50%。抽吸较小的气胸(径向深度 2-3cm 和<2cm)的成功率分别为 82.6%和 100%。
CT-PTLB 后气胸抽气有助于减少约 50%较大气胸患者的胸腔引流管插入,甚至对于较小的气胸(>80%)更是如此。
抽吸最大直径达 3cm 的气胸通常可避免胸腔引流管插入,并可更早出院。