Qiu Wen-Long, Wang Xiao-Lin, Liu Jun-Guang, Hu Gang, Mei Shi-Wen, Tang Jian-Qiang
Department of Colorectal Surgery, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100021, China.
Department of General Surgery, The Second Hospital of Yulin, Yulin 100021, Shaanxi Province, China.
World J Gastrointest Surg. 2023 Jun 27;15(6):1104-1115. doi: 10.4240/wjgs.v15.i6.1104.
Intersphincteric resection (ISR), the ultimate anus-preserving technique for ultralow rectal cancers, is an alternative to abdominoperineal resection (APR). The failure patterns and risk factors for local recurrence and distant metastasis remain controversial and require further investigation.
To investigate the long-term outcomes and failure patterns after laparoscopic ISR in ultralow rectal cancers.
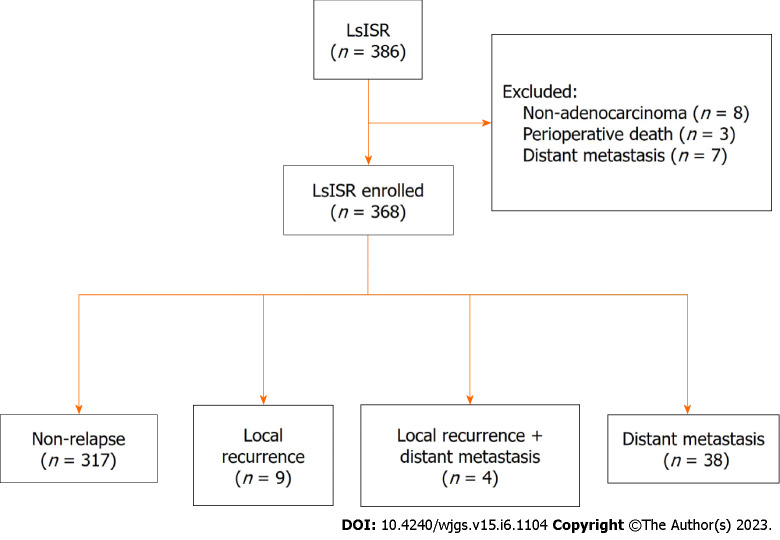
Patients who underwent laparoscopic ISR (LsISR) at Peking University First Hospital between January 2012 and December 2020 were retrospectively reviewed. Correlation analysis was performed using the Chi-square or Pearson's correlation test. Prognostic factors for overall survival (OS), local recurrence-free survival (LRFS), and distant metastasis-free survival (DMFS) were analyzed using Cox regression.
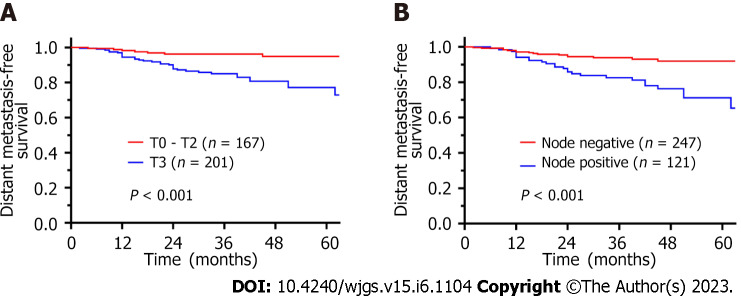
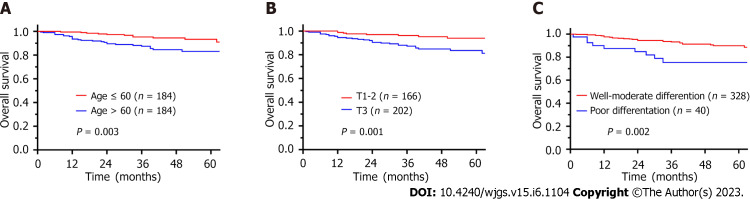
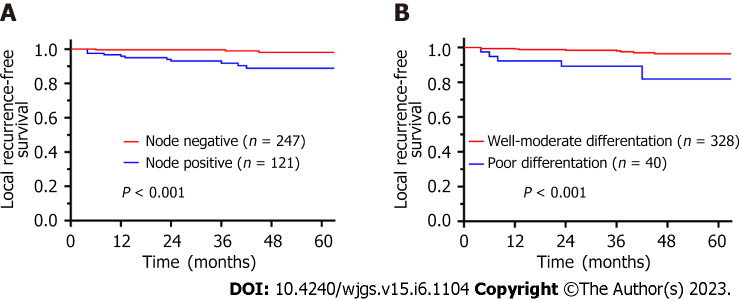
We enrolled 368 patients with a median follow-up of 42 mo. Local recurrence and distant metastasis occurred in 13 (3.5%) and 42 (11.4%) cases, respectively. The 3-year OS, LRFS, and DMFS rates were 91.3%, 97.1%, and 90.1%, respectively. Multivariate analyses revealed that LRFS was associated with positive lymph node status [hazard ratio (HR) = 5.411, 95% confidence interval (CI) = 1.413-20.722, 0.014] and poor differentiation (HR = 3.739, 95%CI: 1.171-11.937, = 0.026), whereas the independent prognostic factors for DMFS were positive lymph node status (HR = 2.445, 95%CI: 1.272-4.698, = 0.007) and (y)pT3 stage (HR = 2.741, 95%CI: 1.225-6.137, = 0.014).
This study confirmed the oncological safety of LsISR for ultralow rectal cancer. Poor differentiation, (y)pT3 stage, and lymph node metastasis are independent risk factors for treatment failure after LsISR, and thus patients with these factors should be carefully managed with optimal neoadjuvant therapy, and for patients with a high risk of local recurrence (N + or poor differentiation), extended radical resection (such as APR instead of ISR) may be more effective.
括约肌间切除术(ISR)是超低位直肠癌保留肛门的终极技术,是腹会阴联合切除术(APR)的替代方案。局部复发和远处转移的失败模式及危险因素仍存在争议,需要进一步研究。
探讨超低位直肠癌腹腔镜ISR术后的长期疗效和失败模式。
回顾性分析2012年1月至2020年12月在北京大学第一医院接受腹腔镜ISR(LsISR)的患者。采用卡方检验或Pearson相关检验进行相关性分析。使用Cox回归分析总生存(OS)、无局部复发生存(LRFS)和无远处转移生存(DMFS)的预后因素。
我们纳入了368例患者,中位随访时间为42个月。局部复发和远处转移分别发生在13例(3.5%)和42例(11.4%)。3年OS、LRFS和DMFS率分别为91.3%、97.1%和90.1%。多因素分析显示,LRFS与阳性淋巴结状态[风险比(HR)=5.411,95%置信区间(CI)=1.413 - 20.722,P = 0.014]和低分化(HR = 3.739,95%CI:1.171 - 11.937,P = 0.026)相关,而DMFS的独立预后因素为阳性淋巴结状态(HR = 2.445,95%CI:1.272 - 4.698,P = 0.007)和(y)pT3期(HR = 所提供原文此处“ = 0.014”前面应该有数字,疑似录入错误,暂按2.741,95%CI:1.225 - 6.137,P = 0.014)。
本研究证实了LsISR治疗超低位直肠癌的肿瘤学安全性。低分化、(y)pT3期和淋巴结转移是LsISR术后治疗失败的独立危险因素,因此对于有这些因素的患者应谨慎采用最佳新辅助治疗,对于局部复发高危患者(N+或低分化),扩大根治性切除(如APR而非ISR)可能更有效。