Department of Cardiology, University Hospital Basel, University of Basel, Petersgraben 4, 4031, Basel, Switzerland.
Cardiovascular Research Institute Basel (CRIB), University Hospital Basel, University of Basel, Basel, Switzerland.
J Nucl Cardiol. 2023 Dec;30(6):2559-2573. doi: 10.1007/s12350-023-03322-3. Epub 2023 Jul 6.
Little is known about the gatekeeper performance of coronary artery calcium score (CACS) before myocardial perfusion positron emission tomography (PET), compared with updated pre-test probabilities from American and European guidelines (pre-test-AHA/ACC, pre-test-ESC).
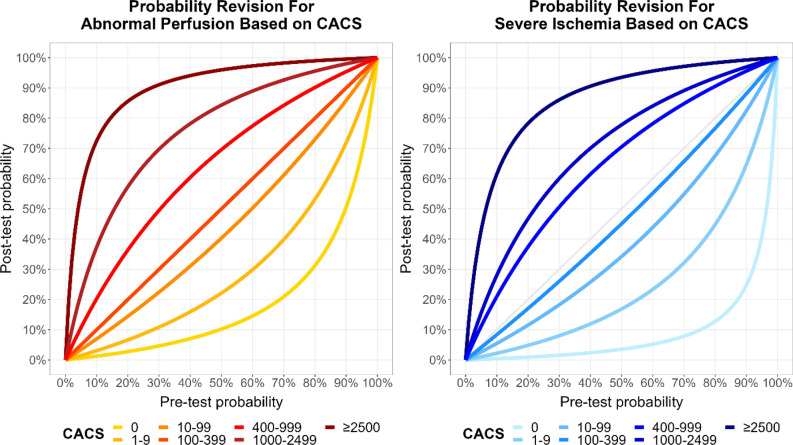
We enrolled participants without known coronary artery disease undergoing CACS and Rubidium-82 PET. Abnormal perfusion was defined as summed stress score ≥ 4. Using Bayes' formula, pre-test probabilities and CACS were combined into post-test probabilities.
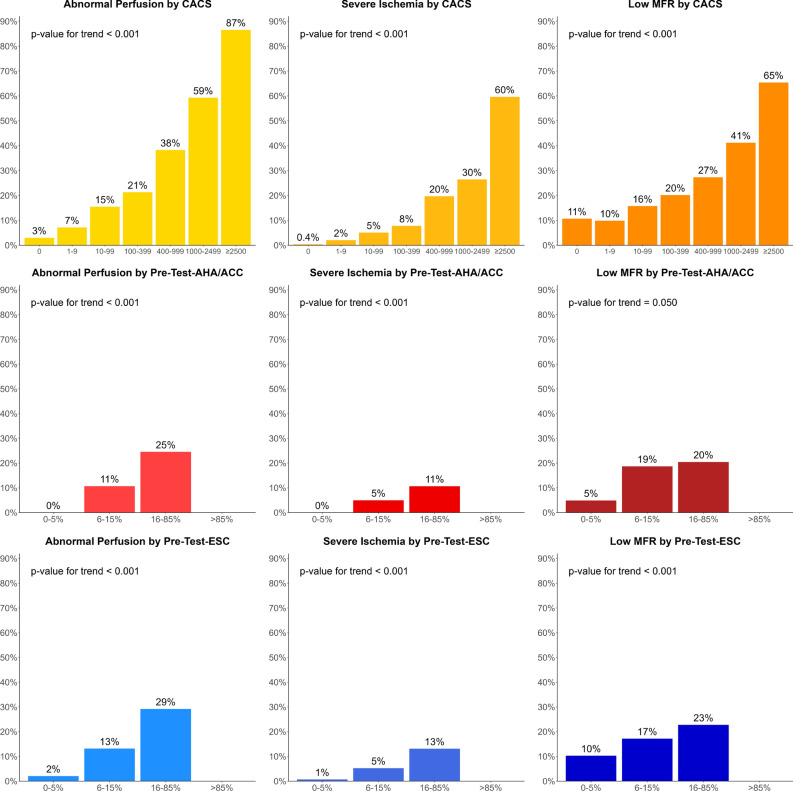
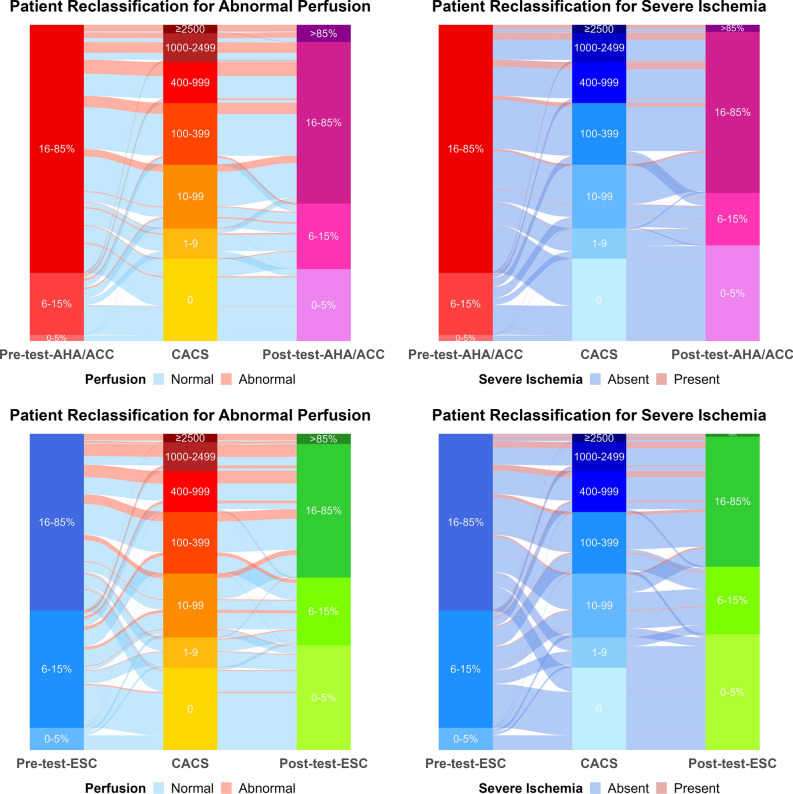
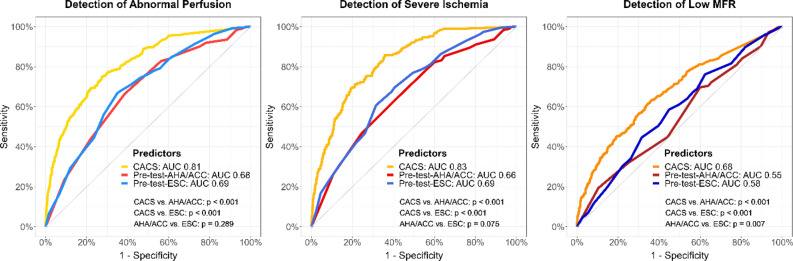
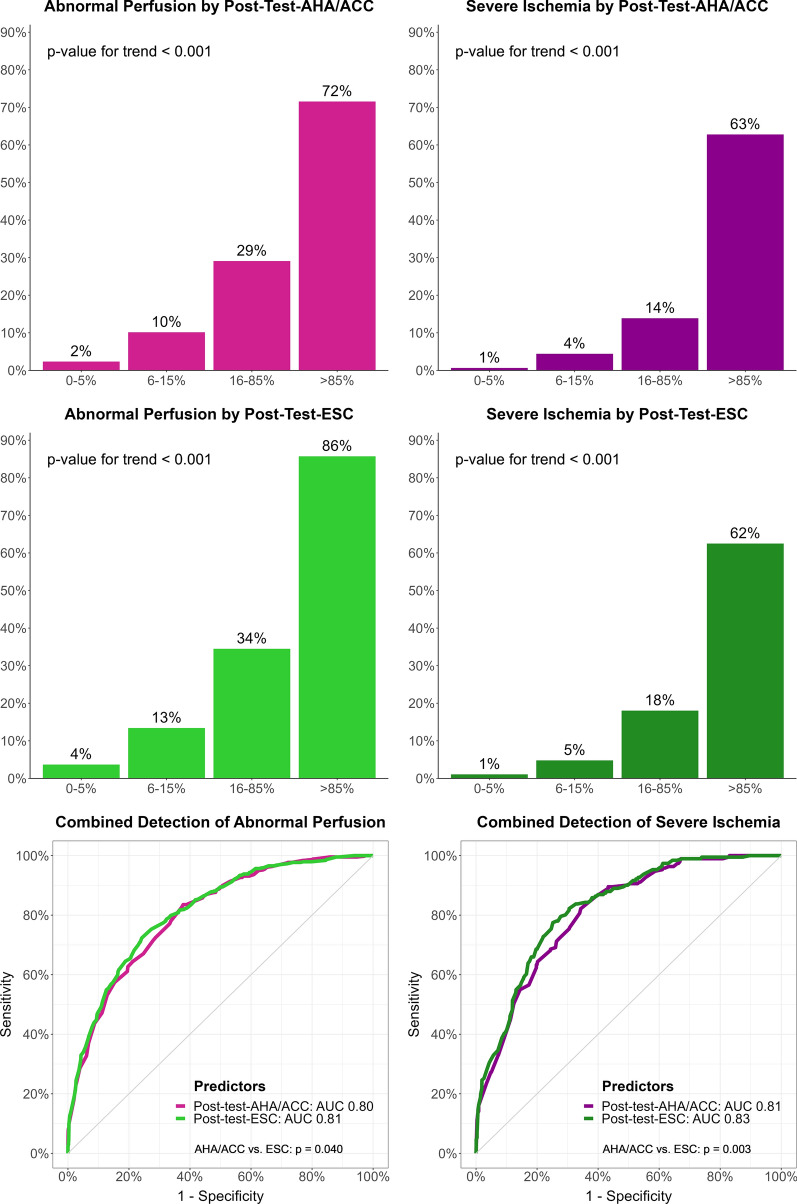
We included 2050 participants (54% male, mean age 64.6 years) with median CACS 62 (IQR 0-380), pre-test-ESC 17% (11-26), pre-test-AHA/ACC 27% (16-44), and abnormal perfusion in 437 participants (21%). To predict abnormal perfusion, area under the curve of CACS was 0.81, pre-test-AHA/ACC 0.68, pre-test-ESC 0.69, post-test-AHA/ACC 0.80, and post-test-ESC 0.81 (P < 0.001 for CACS vs. each pre-test, and each post-test vs. pre-test). CACS = 0 had 97% negative predictive value (NPV), pre-test-AHA/ACC ≤ 5% 100%, pre-test-ESC ≤ 5% 98%, post-test-AHA/ACC ≤ 5% 98%, and post-test-ESC ≤ 5% 96%. Among participants, 26% had CACS = 0, 2% pre-test-AHA/ACC ≤ 5%, 7% pre-test-ESC ≤ 5%, 23% post-test-AHA/ACC ≤ 5%, and 33% post-test-ESC ≤ 5% (all P < 0.001).
CACS and post-test probabilities are excellent predictors of abnormal perfusion and can rule it out with very high NPV in a substantial proportion of participants. CACS and post-test probabilities may be used as gatekeepers before advanced imaging. Coronary artery calcium score (CACS) predicted abnormal perfusion (SSS ≥ 4) in myocardial positron emission tomography (PET) better than pre-test probabilities of coronary artery disease (CAD), while pre-test-AHA/ACC and pre-test-ESC performed similarly (left). Using Bayes' formula, pre-test-AHA/ACC or pre-test-ESC were combined with CACS into post-test probabilities (middle). This calculation reclassified a substantial proportion of participants to low probability of CAD (0-5%), not needing further imaging, as shown for AHA/ACC probabilities (2% with pre-test-AHA/ACC to 23% with post-test-AHA/ACC, P < 0.001, right). Very few participants with abnormal perfusion were classified under pre-test or post-test probabilities 0-5%, or under CACS 0. AUC: area under the curve. Pre-test-AHA/ACC: Pre-test probability of the American Heart Association/American College of Cardiology. Post-test-AHA/ACC: Post-test probability combining pre-test-AHA/ACC and CACS. Pre-test-ESC: Pre-test probability of the European Society of Cardiology. SSS: Summed stress score.
与美国和欧洲指南(预测试-AHA/ACC、预测试-ESC)的更新后的预测试概率相比,冠状动脉钙评分(CACS)在心肌灌注正电子发射断层扫描(PET)之前的门控性能知之甚少。
我们招募了接受 CACS 和放射性铷-82 PET 检查的无已知冠状动脉疾病的参与者。异常灌注定义为总和应激评分≥4。使用贝叶斯公式,将预测试概率和 CACS 结合为后测试概率。
我们纳入了 2050 名参与者(54%为男性,平均年龄 64.6 岁),中位数 CACS 为 62(IQR 0-380),预测试-ESC 为 17%(11-26),预测试-AHA/ACC 为 27%(16-44),437 名参与者存在异常灌注(21%)。为了预测异常灌注,CACS 的曲线下面积为 0.81,预测试-AHA/ACC 为 0.68,预测试-ESC 为 0.69,后测试-AHA/ACC 为 0.80,后测试-ESC 为 0.81(P<0.001 与 CACS 相比,每个预测试和每个后测试与预测试)。CACS=0 时的阴性预测值(NPV)为 97%,预测试-AHA/ACC≤5%时为 100%,预测试-ESC≤5%时为 98%,后测试-AHA/ACC≤5%时为 98%,后测试-ESC≤5%时为 96%。在参与者中,26%的 CACS=0,2%的预测试-AHA/ACC≤5%,7%的预测试-ESC≤5%,23%的后测试-AHA/ACC≤5%,33%的后测试-ESC≤5%(均 P<0.001)。
CACS 和后测试概率是异常灌注的优秀预测指标,在很大一部分参与者中可以非常高的 NPV 排除异常灌注。CACS 和后测试概率可作为高级成像之前的门控。冠状动脉钙评分(CACS)预测心肌正电子发射断层扫描(PET)中的异常灌注(SSS≥4)优于冠状动脉疾病(CAD)的预测试概率,而预测试-AHA/ACC 和预测试-ESC 的表现相似(左图)。使用贝叶斯公式,将预测试-AHA/ACC 或预测试-ESC 与 CACS 结合到后测试概率中(中图)。这种计算将很大一部分参与者重新分类为 CAD 低概率(0-5%),不需要进一步成像,如 AHA/ACC 概率所示(预测试-AHA/ACC 为 2%,后测试-AHA/ACC 为 23%,P<0.001,右图)。很少有异常灌注的参与者被分类为预测试或后测试概率为 0-5%,或 CACS 为 0。AUC:曲线下面积。预测试-AHA/ACC:美国心脏协会/美国心脏病学会的预测试概率。后测试-AHA/ACC:结合预测试-AHA/ACC 和 CACS 的后测试概率。预测试-ESC:欧洲心脏病学会的预测试概率。SSS:总和应激评分。