Amylidi-Mohr Sofia, Wyss Melanie, Surbek Daniel, Raio Luigi, Mosimann Beatrice
Department of Obstetrics, University Hospital of Bern, University of Bern, Bern, Switzerland (Dr Amylidi-Mohr, Ms Wyss, Messrs Surbek and Raio, and Ms Mosimann).
University Hospital of Basel, University of Basel, Basel, Switzerland (Dr Amylidi-Mohr and Ms Mosimann).
AJOG Glob Rep. 2023 Jun 4;3(3):100238. doi: 10.1016/j.xagr.2023.100238. eCollection 2023 Aug.
Gastroschisis and omphalocele are the 2 most common congenital fetal abdominal wall defects. Both malformations are commonly associated with small-for-gestational-age neonates. However, the extent and causes of growth restriction remain controversial in both gastroschisis and omphalocele without associated malformations or aneuploidy.
This study aimed to examine the role of the placenta and the birthweight-to-placental weight ratio in fetuses with abdominal wall defects.
This study included all cases of abdominal wall defects examined at our hospital between January 2001 and December 2020, retrieving the data from the hospital's software. Fetuses with any other combined congenital anomalies, known chromosomal abnormalities, or lost to follow-up were excluded. Overall, 28 singleton pregnancies with gastroschisis and 24 singleton pregnancies with omphalocele met the inclusion criteria. Patient characteristics and pregnancy outcomes were reviewed. The primary outcome was to investigate the association between birthweight and placental weight in pregnancies with abdominal wall defects as measured after delivery. To correct for gestational age and to compare total placental weights, ratios between the observed and expected birthweights for the given gestational age in singletons were calculated. The scaling exponent β was compared with the reference value of 0.75. Statistical analysis was performed using GraphPad Prism (version 8.2.1; GraphPad Software, San Diego, CA) and IBM SPSS Statistics. A value of <.05 indicated statistical significance.
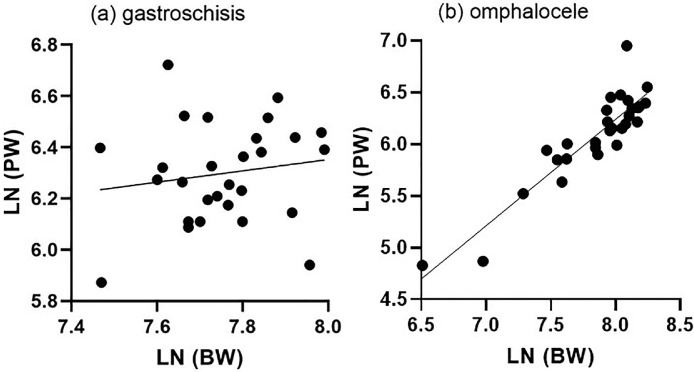
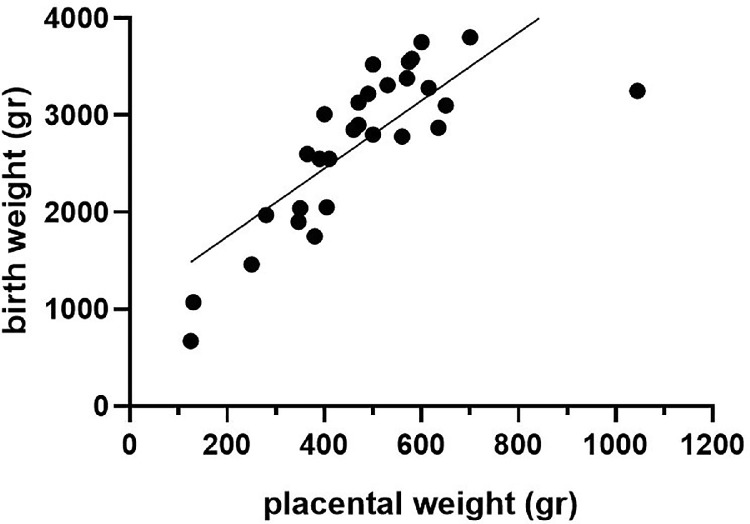
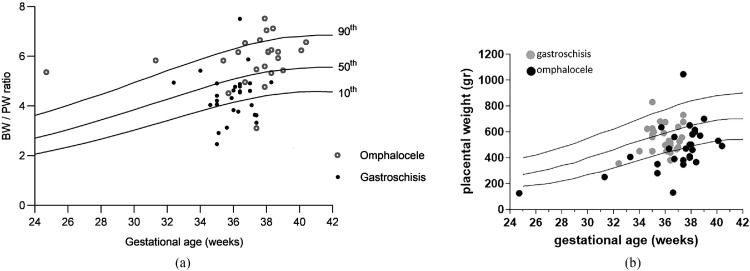
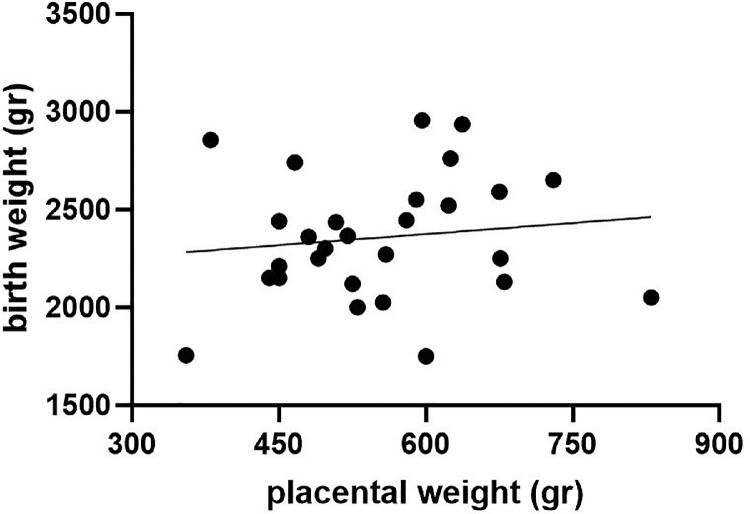
Women pregnant with a fetus with gastroschisis were significantly younger and more often nulliparous. In addition, in this group, the gestational age of delivery was significantly earlier and almost exclusively for cesarean delivery. Of 28 children, 13 (46.7%) were born small for gestational age, only 3 of them (10.7%) had a placental weight <10th percentile. There is no correlation between birthweight percentiles and placental weight percentiles (=not significant). However, in the omphalocele group, 4 of 24 children (16.7%) were born small for gestational age (<10th percentile), and all children also had a placental weight <10th percentile. There is a significant correlation between birthweight percentiles and placental weight percentiles (<.0001). The birthweight-to-placental weight ratio differs significantly between pregnancies diagnosed with gastroschisis and pregnancies diagnosed with omphalocele (4.48 [3.79-4.91] vs 6.05 [5.38-6.47], respectively; <.0001). Allometric metabolic scaling revealed that placentas complicated by gastroschisis and placentas complicated by omphalocele do not scale with birthweight.
Fetuses with gastroschisis displayed impaired intrauterine growth, which seemed to differ from the classical placental insufficiency growth restriction.
腹裂和脐膨出是两种最常见的先天性胎儿腹壁缺陷。这两种畸形通常与小于胎龄儿相关。然而,在无相关畸形或非整倍体的腹裂和脐膨出病例中,生长受限的程度和原因仍存在争议。
本研究旨在探讨胎盘及出生体重与胎盘重量比值在腹壁缺陷胎儿中的作用。
本研究纳入了2001年1月至2020年12月在我院检查的所有腹壁缺陷病例,从医院软件中获取数据。排除有任何其他合并先天性异常、已知染色体异常或失访的胎儿。总体而言,28例单胎妊娠合并腹裂和24例单胎妊娠合并脐膨出符合纳入标准。回顾了患者特征和妊娠结局。主要结局是研究分娩后测量的腹壁缺陷妊娠中出生体重与胎盘重量之间的关联。为校正孕周并比较胎盘总重量,计算了单胎中给定孕周的观察出生体重与预期出生体重的比值。将标度指数β与参考值0.75进行比较。使用GraphPad Prism(版本8.2.1;GraphPad软件,加利福尼亚州圣地亚哥)和IBM SPSS Statistics进行统计分析。P值<0.05表示具有统计学意义。
怀有腹裂胎儿的孕妇明显更年轻,且多为初产妇。此外,在该组中,分娩孕周明显更早,且几乎均为剖宫产。28名儿童中,13名(46.7%)出生时为小于胎龄儿,其中只有3名(10.7%)胎盘重量<第10百分位数。出生体重百分位数与胎盘重量百分位数之间无相关性(P =无显著性)。然而,在脐膨出组中,24名儿童中有4名(16.7%)出生时为小于胎龄儿(<第10百分位数),且所有儿童胎盘重量也<第10百分位数。出生体重百分位数与胎盘重量百分位数之间存在显著相关性(P<0.0001)。诊断为腹裂的妊娠与诊断为脐膨出的妊娠之间的出生体重与胎盘重量比值差异显著(分别为4.48[3.79 - 4.91]和6.05[5.38 - 6.47];P<0.0001)。异速生长代谢标度显示,合并腹裂的胎盘和合并脐膨出的胎盘与出生体重不成比例。
腹裂胎儿表现出宫内生长受损,这似乎与经典的胎盘功能不全性生长受限不同。