Dilley Julian E, Bello Margaret Anne, Roman Natoli, McKinley Todd, Sankar Uma
Department of Orthopaedic Surgery, Indiana University School of Medicine, Indianapolis, IN 46202, USA.
Department of Anatomy, Cell Biology and Physiology, Indiana University School of Medicine, Indianapolis, IN 46202, USA.
Bone Rep. 2023 Jan 30;18:101658. doi: 10.1016/j.bonr.2023.101658. eCollection 2023 Jun.
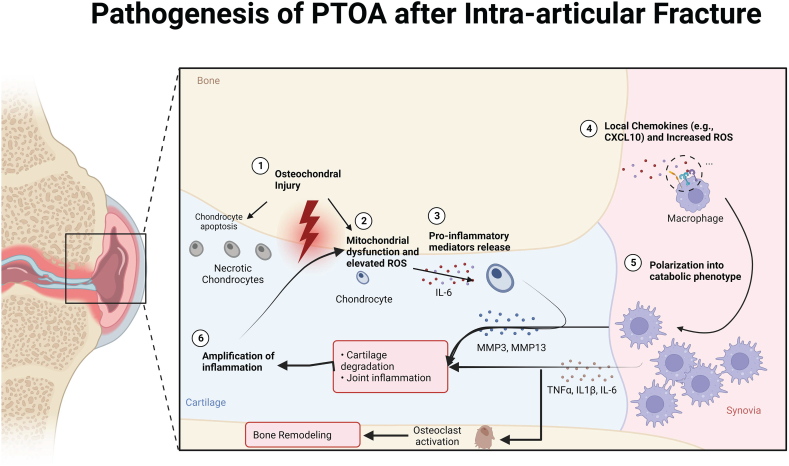
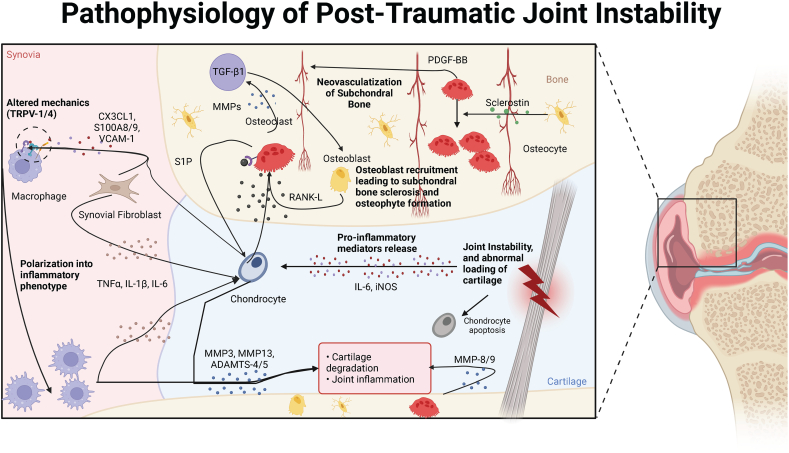
Post-traumatic osteoarthritis (PTOA) develops secondary to a joint injury and accounts for 12 % of all osteoarthritis. These injuries, often of the lower extremity joints, occur due to trauma or accidents related to athletic or military activities. They primarily affect younger individuals although PTOA can occur across the spectrum of age. Pain and functional disability caused by PTOA confer a heavy economic toll on patients, in addition to detrimentally affecting their quality of life. Both high energy injuries that cause articular surface fracture with or without subchondral bone disruption and low-energy injuries involving joint dislocations or ligamentous injury cause PTOA, albeit through different mechanisms. Regardless, chondrocyte death, mitochondrial dysfunction, reactive oxygen species production, subchondral bone remodeling, inflammation and cytokine release in the cartilage and synovium play integral roles in the pathogenesis of PTOA. Evolving surgical methods are focused on stabilizing articular surface and joint structure congruity. However, to date there are no disease modifying medical therapies against PTOA. Increased recent understanding of the pathogenesis of the subchondral bone and synovial inflammation as well as that of chondrocyte mitochondrial dysfunction and apoptosis have led to the investigation of new therapeutics targeting these mechanisms to prevent or delay PTOA. This review discusses new advances in our understanding of cellular mechanisms underlying PTOA, and therapeutic approaches that are potentially effective in reducing the self-propagating cycle of subchondral bone alterations, inflammation, and cartilage degradation. Within this context, we focus therapeutic options involving anti-inflammatory and anti-apoptotic candidates that could prevent PTOA.
创伤后骨关节炎(PTOA)继发于关节损伤,占所有骨关节炎的12%。这些损伤通常发生在下肢关节,是由与体育或军事活动相关的创伤或事故引起的。虽然PTOA可发生于各个年龄段,但主要影响年轻人。PTOA引起的疼痛和功能障碍除了对患者的生活质量产生不利影响外,还给患者带来沉重的经济负担。导致关节面骨折伴或不伴软骨下骨破坏的高能损伤以及涉及关节脱位或韧带损伤的低能损伤均可引起PTOA,尽管其机制不同。无论如何,软骨细胞死亡、线粒体功能障碍、活性氧生成、软骨下骨重塑、炎症以及软骨和滑膜中细胞因子的释放均在PTOA的发病机制中发挥重要作用。不断发展的手术方法主要致力于稳定关节面和关节结构的一致性。然而,迄今为止,尚无针对PTOA的疾病修饰性药物治疗方法。最近对软骨下骨和滑膜炎症发病机制以及软骨细胞线粒体功能障碍和凋亡的认识不断增加,促使人们研究针对这些机制的新疗法,以预防或延缓PTOA。本综述讨论了我们对PTOA潜在细胞机制的新认识,以及可能有效减少软骨下骨改变、炎症和软骨降解的自我传播循环的治疗方法。在此背景下,我们重点介绍了可能预防PTOA的涉及抗炎和抗凋亡候选药物的治疗选择。