Gleditsch Jostein, Jervan Øyvind, Klok Frederikus, Holst René, Hopp Einar, Tavoly Mazdak, Ghanima Waleed
Department of Radiology, Østfold Hospital, Kalnes, Norway.
Institute of Clinical Medicine, University of Oslo Faculty of Medicine, Oslo, Norway.
Acta Radiol Open. 2023 Jun 29;12(6):20584601231187094. doi: 10.1177/20584601231187094. eCollection 2023 Jun.
Rapid diagnosis and risk stratification are important to reduce the risk of adverse clinical events and mortality in acute pulmonary embolism (PE). Although clot burden has not been consistently shown to correlate with disease outcomes, proximally located PE is generally perceived as more severe.
To explore the ability of the Mean Bilateral Proximal Extension of the Clot (MBPEC) score to predict mortality and adverse outcome.
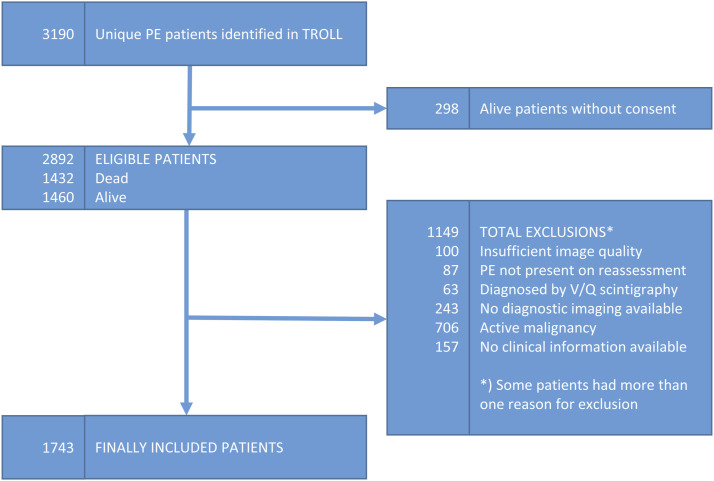
This was a single center retrospective cohort study. 1743 patients with computed tomography pulmonary arteriography (CTPA) verified PE diagnosed between 2005 and 2020 were included. Patients with active malignancy were excluded. The PE clot burden was assessed with MBPEC score: The most proximal extension of PE was scored in each lung from 1 = sub-segmental to 4 = central. The MBPEC score is the score from each lung divided by two and rounded up to nearest integer.
We found inconsistent associations between higher and lower MBPEC scores versus mortality. The all-cause 30-day mortality of 3.9% (95% CI: 3.0-4.9). The PE-related mortality was 2.4% (95% CI: 1.7-3.3). Patients with MBPEC score 1 had higher all-cause mortality compared to patients with MBPEC score 4: Crude Hazard Ratio (cHR) was 2.02 (95% CI: 1.09-3.72). PE-related mortality was lower in patients with MBPEC score 3 compared to score 4: cHR 0.22 (95% CI: 0.05-0.93). Patients with MBPEC score 4 did more often receive systemic thrombolysis compared to patients with MBPEC score 1-3: 3.2% vs. 0.6% ( < .001). Patients with MBPEC score 4 where more often admitted to the intensive care unit: 13% vs. 4.7% ( < .001).
We found no consistent association between the MBPEC score and mortality. Our results therefore indicate that peripheral PE does not necessarily entail a lower morality risk than proximal PE.
快速诊断和风险分层对于降低急性肺栓塞(PE)患者临床不良事件风险和死亡率至关重要。尽管血栓负荷与疾病预后的相关性尚未得到一致证实,但近端肺栓塞通常被认为更为严重。
探讨血栓平均双侧近端延伸(MBPEC)评分预测死亡率和不良结局的能力。
这是一项单中心回顾性队列研究。纳入2005年至2020年间经计算机断层扫描肺动脉造影(CTPA)确诊的1743例肺栓塞患者。排除患有活动性恶性肿瘤的患者。采用MBPEC评分评估肺栓塞血栓负荷:在每侧肺中,将肺栓塞的最近端延伸情况从1分(亚段)至4分(中央型)进行评分。MBPEC评分是每侧肺的评分除以2并向上取整至最接近的整数。
我们发现MBPEC评分高低与死亡率之间的关联并不一致。全因30天死亡率为3.9%(95%置信区间:3.0 - 4.9)。肺栓塞相关死亡率为2.4%(95%置信区间:1.7 - 3.3)。MBPEC评分为1分的患者全因死亡率高于MBPEC评分为4分的患者:粗危险比(cHR)为2.02(95%置信区间:1.09 - 3.72)。MBPEC评分为3分的患者肺栓塞相关死亡率低于评分为4分的患者:cHR为0.22(95%置信区间:0.05 - 0.93)。与MBPEC评分为1 - 3分的患者相比,MBPEC评分为4分的患者接受全身溶栓治疗的频率更高:3.2%对0.6%(P <.001)。MBPEC评分为4分的患者入住重症监护病房的频率更高:13%对4.7%(P <.001)。
我们发现MBPEC评分与死亡率之间没有一致的关联。因此,我们的结果表明,外周型肺栓塞的死亡风险不一定低于近端型肺栓塞。