Winship Cancer Institute of Emory University, Atlanta, GA, USA.
Department of Hematology and Medical Oncology, Emory University School of Medicine, Atlanta, GA, USA.
Oncologist. 2023 Sep 7;28(9):790-798. doi: 10.1093/oncolo/oyad174.
The IMPACT UC I study assessed real-world treatment patterns, outcomes, healthcare resource utilization (HCRU), and costs in patients with metastatic urothelial carcinoma (mUC) receiving first-line (1L) systemic treatment after the FDA approval of 1L immune checkpoint inhibitor (ICI) monotherapy.
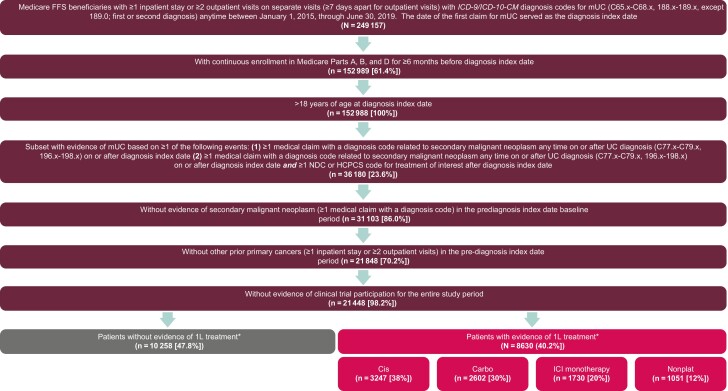
This retrospective study used 100% Medicare fee-for-service claims from 1/1/2015 to 6/30/2019 to identify patients aged ≥18 years diagnosed with UC with evidence of metastatic disease, continuously enrolled for 6 months before and after initial diagnosis. Patients were grouped by 1L treatment: cisplatin-containing chemotherapy, carboplatin-containing chemotherapy, ICI monotherapy, or nonplatinum-containing therapy. Unadjusted time on 1L treatment (TOT), overall survival (OS), HCRU, and total healthcare costs were analyzed.
Of 18 888 patients with mUC, 8630 (45.7%) had received identified 1L systemic treatment; platinum-containing chemotherapy was the most common (cisplatin-containing chemotherapy, 37.6%; carboplatin-containing chemotherapy, 30.2%). Cisplatin- and carboplatin-containing chemotherapy had the shortest time-to-treatment initiation (median, 1.7-3.0 months) and longest TOT (median, 4.0-4.3 months). Median OS was longest with cisplatin-containing chemotherapy (20.0 months) and shortest with ICI monotherapy (7.6 months). Cisplatin- and carboplatin-containing chemotherapy were associated with highest HCRU; total healthcare costs were approximately 2-fold higher with ICI monotherapy vs other 1L treatments ($10 359 vs $5042-$5709 per patient per month).
1L platinum-containing chemotherapy resulted in the longest median OS and highest HCRU, whereas 1L ICI treatment had the shortest median OS and the highest costs. Over 50% of patients diagnosed with advanced UC (aUC) received no systemic therapy, highlighting the importance of optimal 1L treatment decisions in aUC.
IMPACT UC I 研究评估了转移性尿路上皮癌(mUC)患者在接受 FDA 批准的一线(1L)免疫检查点抑制剂(ICI)单药治疗后的真实世界治疗模式、结局、医疗资源利用(HCRU)和成本。
这项回顾性研究使用了 2015 年 1 月 1 日至 2019 年 6 月 30 日 100%的医疗保险按服务收费数据,以确定年龄≥18 岁且有转移性疾病证据的 UC 患者,在初始诊断前和后 6 个月连续入组。患者按 1L 治疗分组:含铂化疗、卡铂化疗、ICI 单药治疗或非铂类治疗。分析了 1L 治疗(TOT)、总生存(OS)、HCRU 和总医疗保健费用的未调整时间。
在 18888 例 mUC 患者中,8630 例(45.7%)接受了明确的 1L 系统治疗;含铂化疗最常见(顺铂化疗,37.6%;卡铂化疗,30.2%)。顺铂和卡铂化疗的治疗起始时间最短(中位数 1.7-3.0 个月),TOT 最长(中位数 4.0-4.3 个月)。含顺铂化疗的中位 OS 最长(20.0 个月),ICI 单药治疗的最短(7.6 个月)。顺铂和卡铂化疗与最高的 HCRU 相关;与其他 1L 治疗(每月每个患者分别为 5042-5709 美元和 10359 美元)相比,ICI 单药治疗的总医疗保健费用约高出 2 倍。
1L 含铂化疗导致中位 OS 最长和最高 HCRU,而 1L ICI 治疗的中位 OS 最短和费用最高。超过 50%的诊断为晚期 UC(aUC)的患者未接受系统治疗,这突出了在 aUC 中进行最佳 1L 治疗决策的重要性。