Tonelli Marcello, Wiebe Natasha, Lunney Meg, Donald Maoliosa, Howarth Tanis, Evans Julie, Klarenbach Scott W, Nicholas David, Boulton Tiffany, Thompson Stephanie, Schick Makaroff Kara, Manns Braden, Hemmelgarn Brenda
Department of Medicine, University of Calgary, Calgary, Canada.
Department of Medicine, University of Alberta, Edmonton, Canada.
EClinicalMedicine. 2023 Jun 29;61:102068. doi: 10.1016/j.eclinm.2023.102068. eCollection 2023 Jul.
Hearing loss (HL) is a leading cause of disability worldwide, but its clinical consequences and population burden have been incompletely studied.
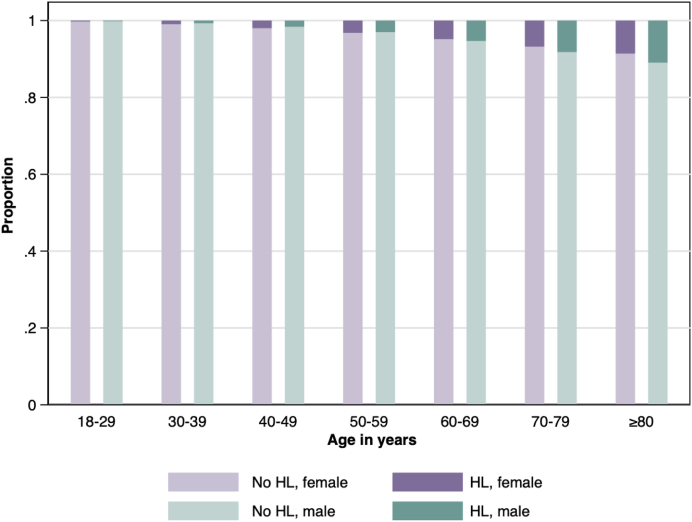
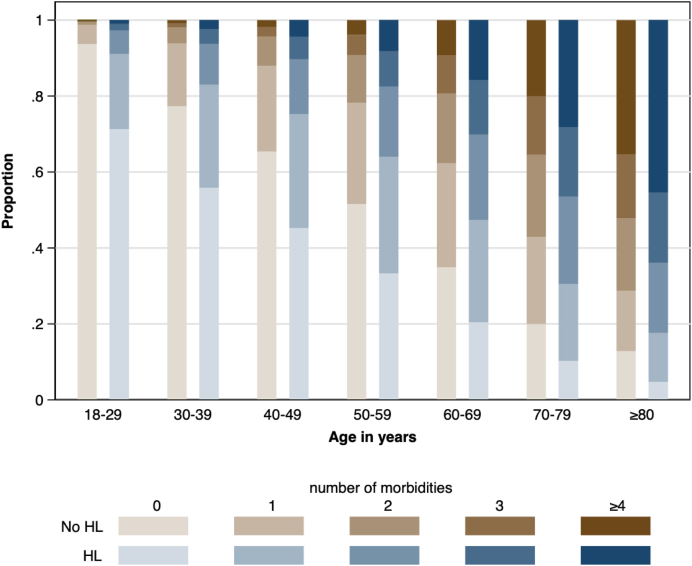
We did a retrospective population-based cohort study of 4,724,646 adults residing in Alberta between April 1, 2004 and March 31, 2019, of whom 152,766 (3.2%) had HL identified using administrative health data. We used administrative data to identify comorbidity and clinical outcomes, including death, myocardial infarction, stroke/transient ischemic attack, depression, dementia, placement in long-term care (LTC), hospitalization, emergency visits, pressure ulcers, adverse drug events and falls. We used Weibull survival models (binary outcomes) and negative binomial models (rate outcomes) to compare the likelihood of outcomes in those with vs without HL. We calculated population-attributable fractions to estimate the number of binary outcomes associated with HL.
The age-sex-standardized prevalence of all 31 comorbidities at baseline was higher among participants with HL than those without. Over median follow-up of 14.4 y and after adjustment for potential confounders at baseline, participants with HL had higher rates of days in hospital (rate ratio 1.65, 95% CI 1.39, 1.97), falls (RR 1.72, 95% CI 1.59, 1.86), adverse drug events (RR 1.40, 95% CI 1.35, 1.45), and emergency visits (RR 1.21, 95% CI 1.14, 1.28) compared to those without, and higher adjusted hazards of death, myocardial infarction, stroke/transient ischemic attack, depression, heart failure, dementia, pressure ulcers and LTC placement. The estimated number of people with HL who required new LTC placement annually in Canada was 15,631, of which 1023 were attributable to HL. Corresponding estimates for new dementia among people with HL were 14,959 and 4350, and for stroke/TIA the estimates were 11,582 and 2242.
HL is common, is often accompanied by substantial comorbidity, and is associated with significant increases in risk for a broad range of adverse clinical outcomes, some of which are potentially preventable. This high population health burden suggests that increased and coordinated investment is needed to improve the care of people with HL.
Canadian Institutes of Health Research; David Freeze chair in health services research.
听力损失(HL)是全球致残的主要原因之一,但其临床后果和人群负担尚未得到充分研究。
我们对2004年4月1日至2019年3月31日居住在艾伯塔省的4,724,646名成年人进行了一项基于人群的回顾性队列研究,其中152,766人(3.2%)通过行政卫生数据被确定患有HL。我们使用行政数据来确定合并症和临床结局,包括死亡、心肌梗死、中风/短暂性脑缺血发作、抑郁症、痴呆症、长期护理(LTC)安置、住院、急诊就诊、压疮、药物不良事件和跌倒。我们使用威布尔生存模型(二元结局)和负二项式模型(发生率结局)来比较有HL和无HL者发生结局的可能性。我们计算人群归因分数以估计与HL相关的二元结局数量。
在基线时,所有31种合并症的年龄性别标准化患病率在有HL参与者中高于无HL者。在中位随访14.4年并对基线潜在混杂因素进行调整后,与无HL者相比,有HL参与者的住院天数发生率更高(发生率比1.65,95%CI 1.39,1.97)、跌倒发生率更高(RR 1.72,95%CI 1.59,1.86)、药物不良事件发生率更高(RR 1.40,95%CI 1.35,1.45)以及急诊就诊发生率更高(RR 1.21,95%CI 1.14,1.28),并且死亡、心肌梗死、中风/短暂性脑缺血发作、抑郁症、心力衰竭、痴呆症、压疮和LTC安置的调整后风险更高。在加拿大,估计每年需要新安置LTC的HL患者人数为15,631人,其中1023人可归因于HL。HL患者中新发痴呆症的相应估计人数分别为14,959人和4350人,中风/TIA的估计人数分别为11,582人和2242人。
HL很常见,常伴有大量合并症,并与广泛不良临床结局的风险显著增加相关,其中一些结局可能是可预防的。这种高人群健康负担表明需要增加并协调投资以改善HL患者的护理。
加拿大卫生研究院;大卫·弗里兹卫生服务研究主席职位。