Alamoodi Munaser, Wazir Umar, Mokbel Kinan, Patani Neill, Varghese Jajini, Mokbel Kefah
Faculty of Medicine, King Abdulaziz University, Jeddah 21589, Saudi Arabia.
The London Breast Institute, Princess Grace Hospital, London W1U 5NY, UK.
Cancers (Basel). 2023 Jun 24;15(13):3325. doi: 10.3390/cancers15133325.
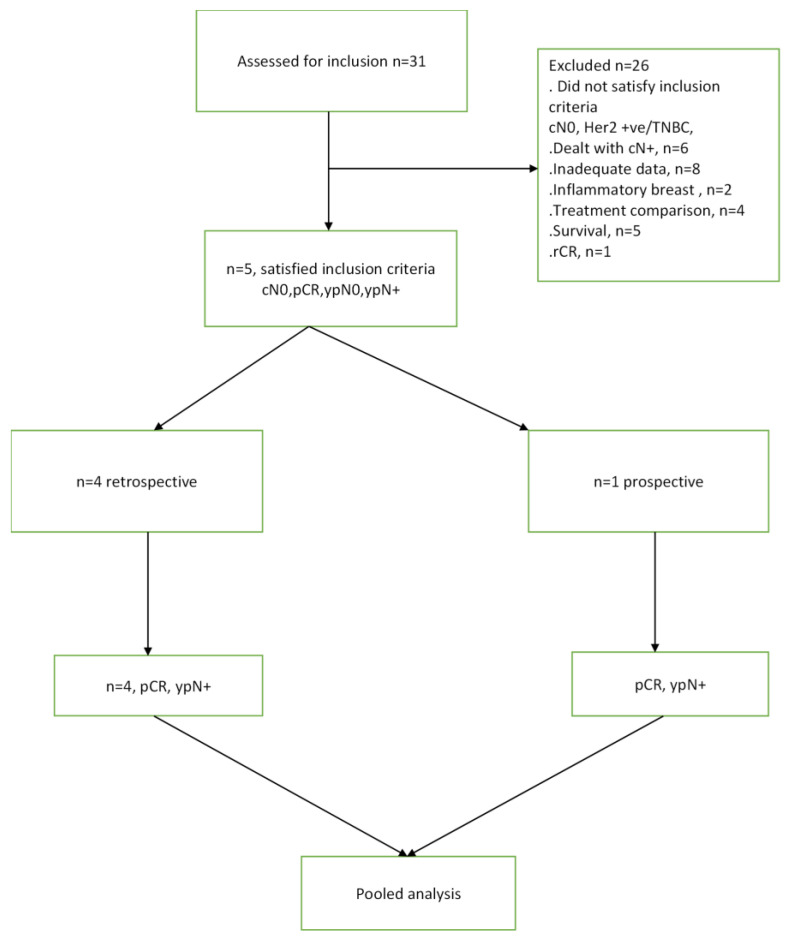
Recent advances in systemic treatment for breast cancer have been underpinned by recognising and exploiting subtype-specific vulnerabilities to achieve higher rates of pathologic complete response (pCR) after neo-adjuvant systemic therapy (NAST). This down-staging of disease has permitted safe surgical de-escalation in patients who respond well. Triple-negative (TNBC) or HER2-positive breast cancer is most likely to achieve complete radiological response (rCR) and pCR after NAST. Hence, for selected patients, particularly those who are clinically node-negative (cN0) at diagnosis, the probability of disease in the sentinel node after NAST could be low enough to justify omitting axillary surgery. The aim of this pooled analysis was to determine the rate of sentinel node positivity (ypN+) in patients with TNBC or HER2-positive breast cancer who were initially cN0, achieving rCR and/or pCR in the breast after NAST. MedLine was searched using appropriate search terms. Five studies (N = 3834) were included in the pooled analysis, yielding a pooled ypN+ rate of 2.16% (95% CI: 1.70-2.63). This is significantly lower than the acceptable false negative rate of sentinel lymph node biopsy (SLNB) and supports consideration of omission of SLNB in this subset of patients.
乳腺癌全身治疗的最新进展基于识别和利用亚型特异性弱点,以在新辅助全身治疗(NAST)后实现更高的病理完全缓解(pCR)率。疾病的这种降期使得对反应良好的患者能够安全地缩小手术范围。三阴性(TNBC)或HER2阳性乳腺癌在NAST后最有可能实现完全放射学缓解(rCR)和pCR。因此,对于选定的患者,尤其是那些诊断时临床淋巴结阴性(cN0)的患者,NAST后前哨淋巴结中出现疾病的可能性可能低到足以证明可以省略腋窝手术。这项汇总分析的目的是确定最初为cN0、在NAST后乳腺实现rCR和/或pCR的TNBC或HER2阳性乳腺癌患者的前哨淋巴结阳性率(ypN+)。使用适当的检索词对MedLine进行了检索。五项研究(N = 3834)纳入了汇总分析,汇总ypN+率为2.16%(95%CI:1.70 - 2.63)。这显著低于前哨淋巴结活检(SLNB)可接受的假阴性率,并支持考虑在这部分患者中省略SLNB。