Spautz Saskia, Haase Leon, Tschiche Maria, Makocki Sebastian, Richter Christian, Troost Esther G C, Stützer Kristin
OncoRay - National Center for Radiation Research in Oncology, Faculty of Medicine and University Hospital Carl Gustav Carus, Technische Universität Dresden, Helmholtz-Zentrum Dresden, Rossendorf, Fetscherstraße 74, PF 41, 01307 Dresden, Germany.
Department of Radiotherapy and Radiation Oncology, Faculty of Medicine and University Hospital Carl Gustav Carus, Technische Universität Dresden, Fetscherstraße 74, PF 50, 01307 Dresden, Germany.
Phys Imaging Radiat Oncol. 2023 Jun 24;27:100465. doi: 10.1016/j.phro.2023.100465. eCollection 2023 Jul.
There is no consensus about an ideal robust optimization (RO) strategy for proton therapy of targets with large intrafractional motion. We investigated the plan robustness of 3D and different 4D RO strategies.
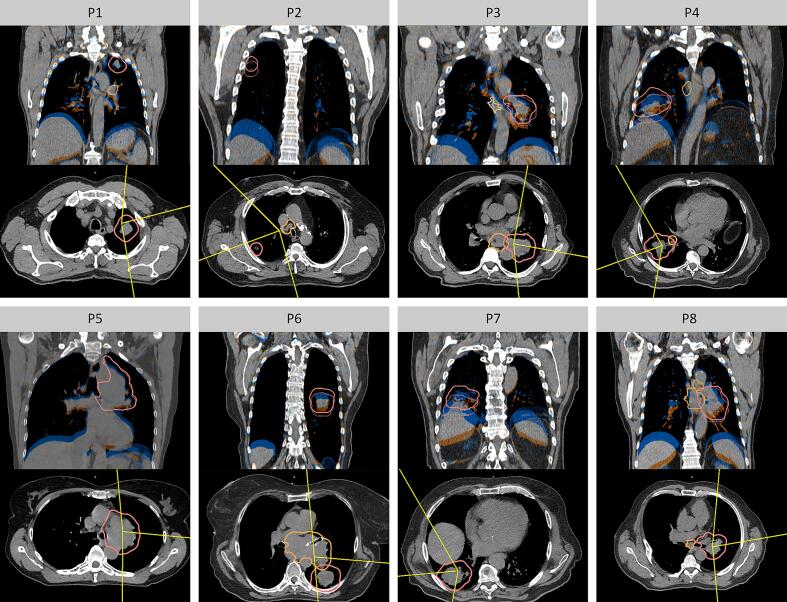
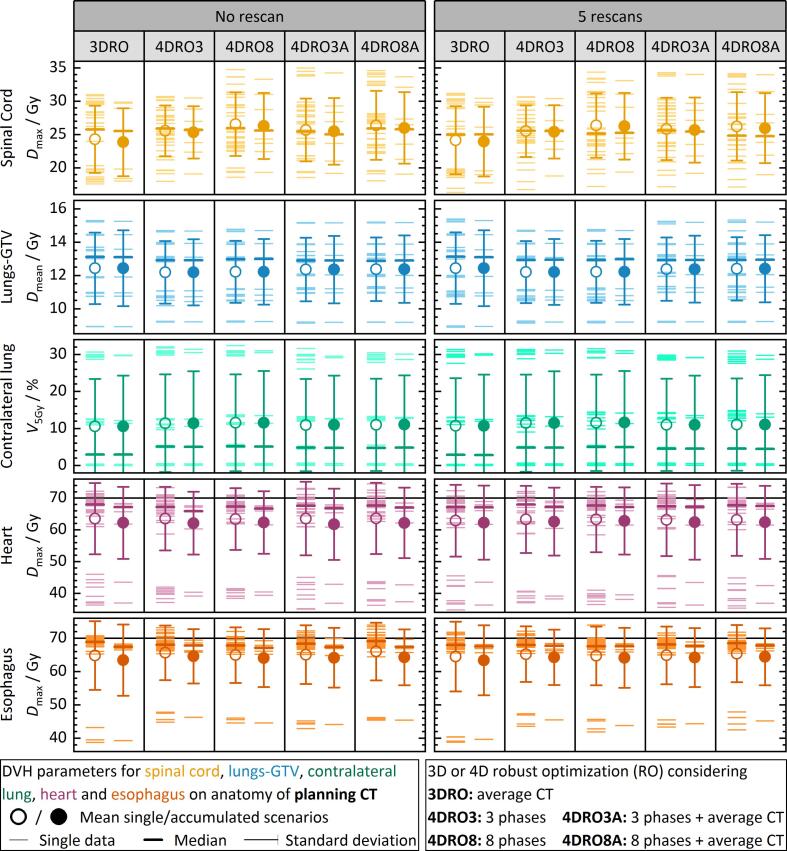
For eight non-small cell lung cancer patients with clinical target volume (CTV) motion >5 mm, different RO approaches were investigated: 3DRO considering the average CT (AvgCT) with a target density override, 4DRO considering three/all 4DCT phases, and 4DRO considering the AvgCT and three/all 4DCT phases. Robustness against setup/range errors, interplay effects based on breathing and machine log file data for deliveries with/without rescanning, and interfractional anatomical changes were analyzed for target coverage and OAR sparing.
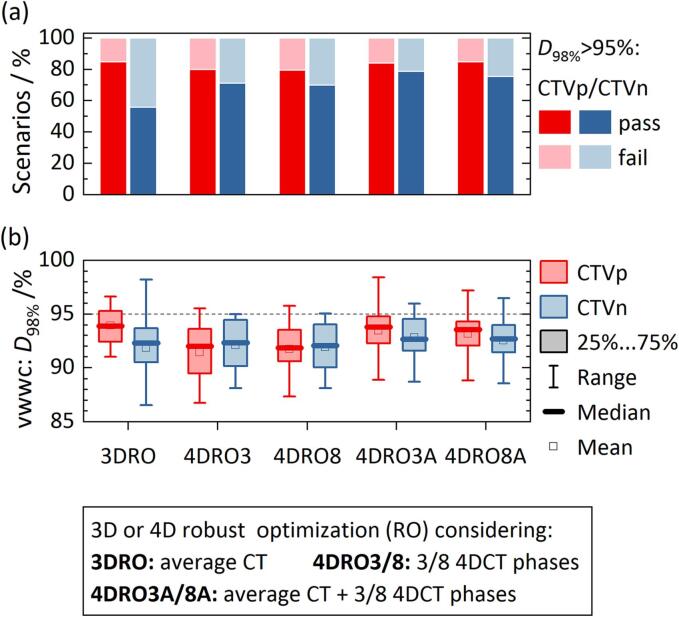
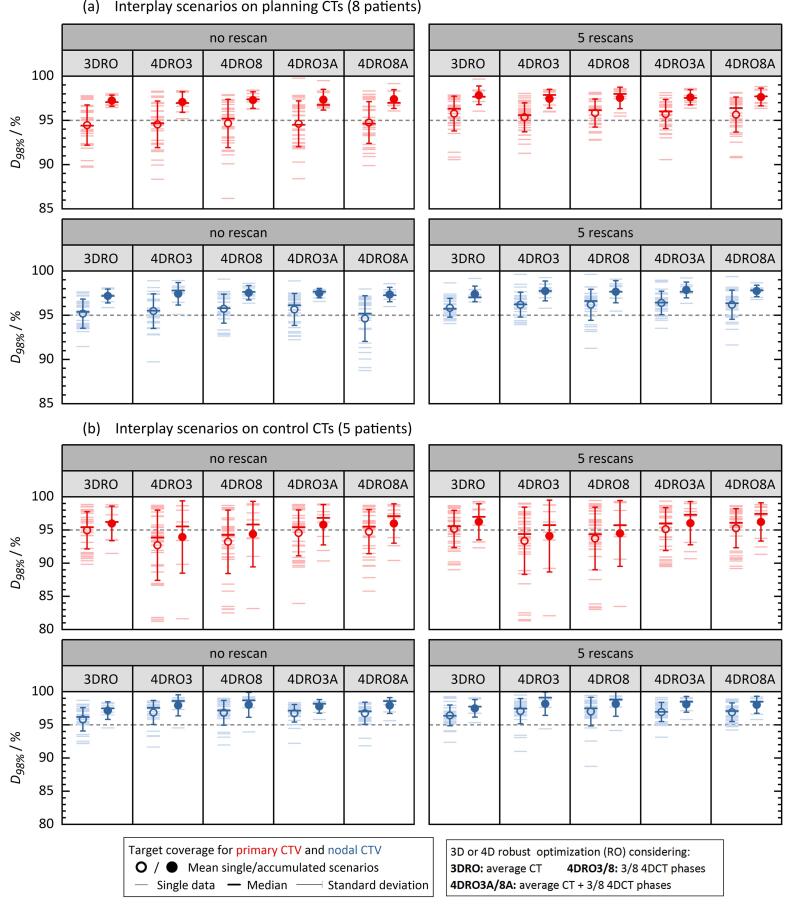
All nominal plans fulfilled the clinical requirements with individual CTV coverage differences <2pp; 4DRO without AvgCT generated the most conformal dose distributions. Robustness against setup/range errors was best for 4DRO with AvgCT (18% more passed error scenarios than 3DRO). Interplay effects caused fraction-wise median CTV coverage loss of 3pp and missed maximum dose constraints for heart and esophagus in 18% of scenarios. CTV coverage and OAR sparing fulfilled requirements in all cases when accumulating four interplay scenarios. Interfractional changes caused less target misses for RO with AvgCT compared to 4DRO without AvgCT (≤42%/33% vs. ≥56%/44% failed single/accumulated scenarios).
All RO strategies provided acceptable plans with equally low robustness against interplay effects demanding other mitigation than rescanning to ensure fraction-wise target coverage. 4DRO considering three phases and the AvgCT provided best compromise on planning effort and robustness.
对于具有较大分次内运动的靶区进行质子治疗,目前尚无关于理想的稳健优化(RO)策略的共识。我们研究了三维(3D)和不同的四维(4D)RO策略的计划稳健性。
对于八名临床靶体积(CTV)运动>5mm的非小细胞肺癌患者,研究了不同的RO方法:考虑平均CT(AvgCT)并覆盖靶区密度的3DRO、考虑三个/所有4DCT时相的4DRO,以及考虑AvgCT和三个/所有4DCT时相的4DRO。分析了针对摆位/射程误差的稳健性、基于呼吸的相互作用效应以及有无重新扫描时机器日志文件数据的分次照射情况,以及分次间解剖结构变化对靶区覆盖和危及器官(OAR)保护的影响。
所有标称计划均满足临床要求,个体CTV覆盖差异<2个百分点;不考虑AvgCT的4DRO产生了最适形的剂量分布。对于考虑AvgCT的4DRO,针对摆位/射程误差的稳健性最佳(比3DRO多18%的误差情况通过)。相互作用效应导致分次中位CTV覆盖损失3个百分点,在18%的情况下心脏和食管的最大剂量约束未达标。累积四种相互作用情况时,CTV覆盖和OAR保护在所有情况下均满足要求。与不考虑AvgCT的4DRO相比,考虑AvgCT的RO分次间变化导致的靶区遗漏更少(单次/累积情况失败的比例分别为≤42%/33% 与≥56%/44%)。
所有RO策略均提供了可接受的计划,对于相互作用效应的稳健性同样较低,需要除重新扫描之外的其他缓解措施以确保分次靶区覆盖。考虑三个时相和AvgCT的4DRO在计划工作量和稳健性方面提供了最佳折衷方案。