Department of Cardiovascular Medicine, Wakayama Medical University, Wakayama, Japan.
Department of Cardiovascular Medicine, Kyoto Prefectural University of Medicine, Kyoto, Japan.
Sci Rep. 2023 Jul 17;13(1):11544. doi: 10.1038/s41598-023-38578-9.
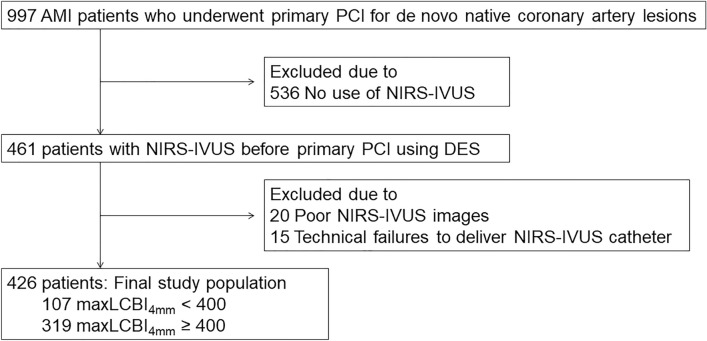
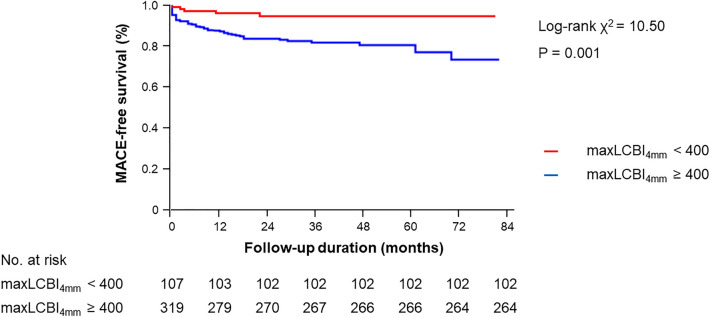
Acute myocardial infarction (AMI) can rarely arise from non-lipid-rich coronary plaques. This study sought to compare the clinical outcomes after percutaneous coronary intervention (PCI) between AMI showing maximum lipid-core burden index in 4 mm (maxLCBI) < 400 and ≥ 400 in the infarct-related lesions assessed by near-infrared spectroscopy-intravascular ultrasound (NIRS-IVUS). We investigated 426 AMI patients who underwent NIRS-IVUS in the infarct-related lesions before PCI. Major adverse cardiovascular events (MACE) were defined as the composite of cardiac death, non-fatal MI, clinically driven target lesion revascularization (TLR), clinically driven non-TLR, and congestive heart failure requiring hospitalization. 107 (25%) patients had infarct-related lesions of maxLCBI < 400, and 319 (75%) patients had those of maxLCBI ≥ 400. The maxLCBI < 400 group had a younger median age at onset (68 years [IQR: 57-78 years] vs. 73 years [IQR: 64-80 years], P = 0.007), less frequent multivessel disease (39% vs. 51%, P = 0.029), less frequent TIMI flow grade 0 or 1 before PCI (62% vs. 75%, P = 0.007), and less frequent no-reflow immediately after PCI (5% vs. 11%, P = 0.039). During a median follow-up period of 31 months [IQR: 19-48 months], the frequency of MACE was significantly lower in the maxLCBI < 400 group compared with the maxLCBI ≥ 400 group (4.7% vs. 17.2%, P = 0.001). MaxLCBI < 400 was an independent predictor of MACE-free survival at multivariable analysis (hazard ratio: 0.36 [confidence interval: 0.13-0.98], P = 0.046). MaxLCBI < 400 measured by NIRS in the infract-related lesions before PCI was associated with better long-term clinical outcomes in AMI patients.
急性心肌梗死(AMI)很少由富含脂质的冠状动脉斑块引起。本研究旨在比较经皮冠状动脉介入治疗(PCI)后梗死相关病变中最大脂质核心负荷指数(maxLCBI)<400 和≥400 的 AMI 患者的临床预后。我们研究了 426 例在 PCI 前接受近红外光谱血管内超声(NIRS-IVUS)评估的梗死相关病变的 AMI 患者。主要不良心血管事件(MACE)定义为心脏死亡、非致死性心肌梗死、临床驱动的靶病变血运重建(TLR)、临床驱动的非 TLR 和需要住院的充血性心力衰竭的复合事件。107 例(25%)患者梗死相关病变的 maxLCBI<400,319 例(75%)患者梗死相关病变的 maxLCBI≥400。maxLCBI<400 组的发病中位年龄更年轻(68 岁[IQR:57-78 岁] vs. 73 岁[IQR:64-80 岁],P=0.007),多支血管病变频率更低(39% vs. 51%,P=0.029),PCI 前 TIMI 血流分级 0 或 1 频率更低(62% vs. 75%,P=0.007),PCI 后即刻无复流频率更低(5% vs. 11%,P=0.039)。在中位随访 31 个月[IQR:19-48 个月]期间,maxLCBI<400 组的 MACE 发生率明显低于 maxLCBI≥400 组(4.7% vs. 17.2%,P=0.001)。多变量分析显示,maxLCBI<400 是 MACE 无复发生存的独立预测因子(危险比:0.36[置信区间:0.13-0.98],P=0.046)。PCI 前 NIRS 测量的梗死相关病变中的 maxLCBI<400 与 AMI 患者的长期临床预后较好相关。