Department for Diagnostic and Interventional Radiology, University Hospital Tuebingen, Hoppe-Seyler-Strasse 3, Tuebingen, 72076, Germany.
Department for Radiology, Diakonieklinikum Stuttgart, Stuttgart, Germany.
BMC Gastroenterol. 2023 Jul 17;23(1):241. doi: 10.1186/s12876-023-02876-3.
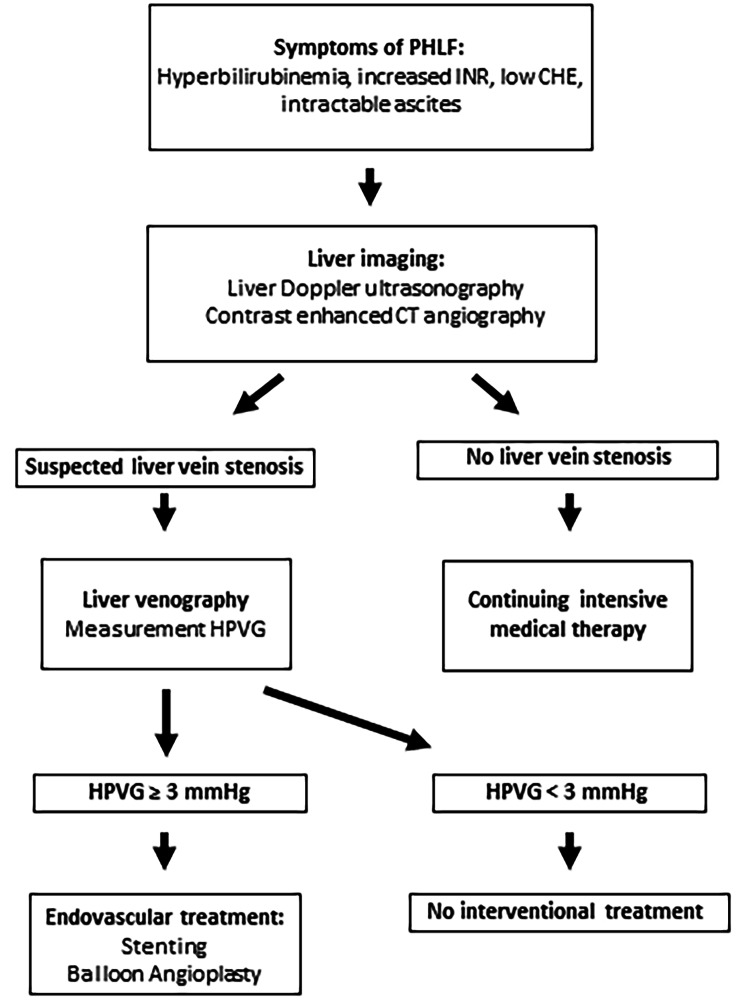
To evaluate efficacy, safety, and outcomes of endovascular treatment of hepatic vein stenosis post major liver resection.
A retrospective data analysis was performed including all interventional treatments of hepatic vein stenosis post major liver resection since 2010. Post procedural course and clinical parameters including amount of ascites accumulation and relevant laboratory values were assessed during the follow-up period. Primary and primary assisted hepatic venous patency time were calculated.
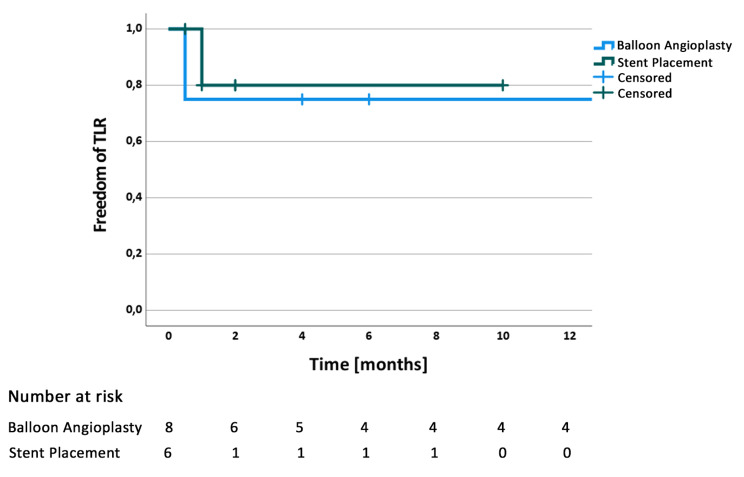
Twelve patients (median age 55.5, IQR 49.75 to 61.5 years) undergoing a total of 16 interventions were included. Interventions were primary stent placement (n = 3), primary balloon angioplasty (n = 8), three re-interventions and two aborted interventions (no significant pressure gradient). Technical success was 100% (16/16). Permanent reduction and / or complete resolution of ascites was achieved in 72% (8/11). Laboratory parameters related to liver function did not show significant improvement after intervention. Median follow-up period was 6 months (IQR: 1.5 to 18 months). The median primary patency time for patients with balloon angioplasty was 11 months (IQR: 1.375 to 22.25 months) and assisted patency time was 13.25 months (IQR: 4.5 to 22.25 months). The median primary patency time for patients with angioplasty and stent placement was 1 months (IQR: 1.0 to 1.5 months) and assisted patency time was 2.0 months (IQR: 1.5 to 2.5months).
An endovascular approach for the treatment of hepatic venous stenosis post major liver resection is safe and efficient to reduce and / or resolve refractory ascites. However, liver function parameters seem not to be improved by the procedure. Stent placement can be a reasonable option in patients with significant residual stenotic disease post angioplasty.
评估肝切除术治疗肝静脉狭窄的疗效、安全性和结果。
对 2010 年以来所有肝切除术治疗肝静脉狭窄的介入治疗进行回顾性数据分析。在随访期间评估术后过程和临床参数,包括腹水积聚量和相关实验室值。计算主要和辅助肝静脉通畅时间。
共纳入 12 例(中位年龄 55.5 岁,IQR 49.75-61.5 岁)患者,共行 16 次介入治疗。介入治疗包括初次支架置入(n=3)、初次球囊血管成形术(n=8)、3 次再介入和 2 次放弃干预(无明显压力梯度)。技术成功率为 100%(16/16)。72%(8/11)的患者腹水永久性减少和/或完全缓解。干预后肝功能相关实验室参数无明显改善。中位随访时间为 6 个月(IQR:1.5-18 个月)。球囊血管成形术患者的中位初次通畅时间为 11 个月(IQR:1.375-22.25 个月),辅助通畅时间为 13.25 个月(IQR:4.5-22.25 个月)。血管成形术和支架置入患者的中位初次通畅时间为 1 个月(IQR:1.0-1.5 个月),辅助通畅时间为 2.0 个月(IQR:1.5-2.5 个月)。
肝切除术治疗肝静脉狭窄后,血管内治疗可安全有效地减少和/或消除难治性腹水。然而,该手术似乎不能改善肝功能参数。对于血管成形术后仍有明显残余狭窄的患者,支架置入可能是一种合理的选择。