Pirie Katrina P, Wang Andy, Yu Joanna, Teng Bao, Doane Matthew A, Myles Paul S, Riedel Bernhard
Department of Anaesthesiology and Perioperative Medicine, Alfred Hospital, Melbourne, Australia.
Central Clinical School, Monash University, Melbourne, Australia.
Perioper Med (Lond). 2023 Jul 18;12(1):40. doi: 10.1186/s13741-023-00324-0.
Thoracic epidural analgesia is commonly used for upper gastrointestinal surgery. Intrathecal morphine is an appealing opioid-sparing non-epidural analgesic option, especially for laparoscopic gastrointestinal surgery.
Following ethics committee approval, we extracted data from the electronic medical records of patients at Royal North Shore Hospital (Sydney, Australia) that had upper gastrointestinal surgery between November 2015 and October 2020. Postoperative morphine consumption and pain scores were modelled with a Bayesian mixed effect model.
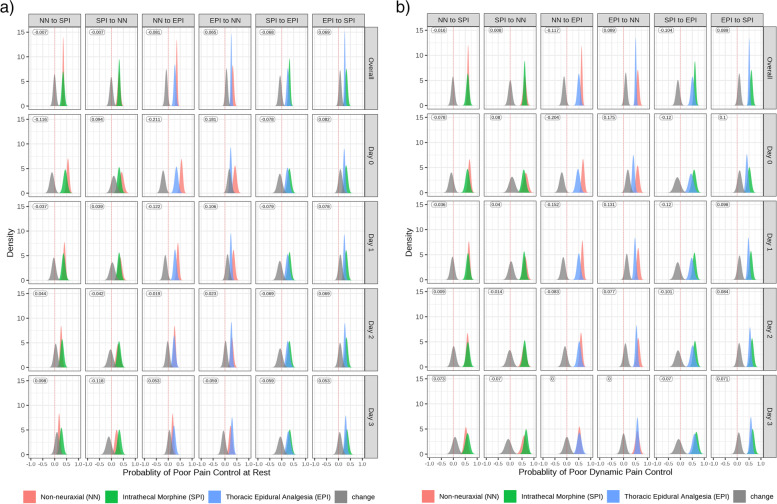
A total of 427 patients were identified who underwent open (n = 300), laparoscopic (n = 120) or laparoscopic converted to open (n = 7) upper gastrointestinal surgery. The majority of patients undergoing open surgery received a neuraxial technique (thoracic epidural [58%, n = 174]; intrathecal morphine [21%, n = 63]) compared to a minority in laparoscopic approaches (thoracic epidural [3%, n = 4]; intrathecal morphine [12%, n = 14]). Intrathecal morphine was superior over non-neuraxial analgesia in terms of lower median oral morphine equivalent consumption and higher probability of adequate pain control; however, this effect was not sustained beyond postoperative day 2. Thoracic epidural analgesia was superior to both intrathecal and non-neuraxial analgesia options for both primary outcomes, but at the expense of higher rates of postoperative hypotension (60%, n = 113) and substantial technique failure rates (32%).
We found that thoracic epidural analgesia was superior to intrathecal morphine, and intrathecal morphine was superior to non-neuraxial analgesia, in terms of reduced postoperative morphine requirements and the probability of adequate pain control in patients who underwent upper gastrointestinal surgery. However, the benefits of thoracic epidural analgesia and intrathecal morphine were not sustained across all time periods regarding control of pain. The study is limited by its retrospective design, heterogenous group of upper gastrointestinal surgeries and confounding by indication.
胸段硬膜外镇痛常用于上消化道手术。鞘内注射吗啡是一种有吸引力的节省阿片类药物的非硬膜外镇痛选择,尤其适用于腹腔镜胃肠道手术。
经伦理委员会批准后,我们从澳大利亚悉尼皇家北岸医院2015年11月至2020年10月期间接受上消化道手术患者的电子病历中提取数据。术后吗啡消耗量和疼痛评分采用贝叶斯混合效应模型进行建模。
共识别出427例接受开放手术(n = 300)、腹腔镜手术(n = 120)或腹腔镜中转开放手术(n = 7)的上消化道手术患者。与腹腔镜手术中的少数患者(胸段硬膜外[3%,n = 4];鞘内注射吗啡[12%,n = 14])相比,大多数接受开放手术的患者接受了神经轴技术(胸段硬膜外[58%,n = 174];鞘内注射吗啡[21%,n = 63])。鞘内注射吗啡在较低的口服吗啡当量中位数消耗量和充分疼痛控制的较高概率方面优于非神经轴镇痛;然而,这种效果在术后第2天之后未持续。胸段硬膜外镇痛在两个主要结局方面均优于鞘内和非神经轴镇痛选择,但代价是术后低血压发生率较高(60%,n = 113)和技术失败率较高(32%)。
我们发现,就减少上消化道手术患者术后吗啡需求量和充分疼痛控制的概率而言,胸段硬膜外镇痛优于鞘内注射吗啡,鞘内注射吗啡优于非神经轴镇痛。然而,胸段硬膜外镇痛和鞘内注射吗啡在疼痛控制的所有时间段内的益处并未持续。本研究受其回顾性设计、上消化道手术的异质性组以及指征混杂的限制。