GSK, Durham, North Carolina, USA.
Leiden Experts on Advanced Pharmacokinetics and Pharmacodynamics, Leiden, The Netherlands.
CPT Pharmacometrics Syst Pharmacol. 2023 Oct;12(10):1411-1424. doi: 10.1002/psp4.13016. Epub 2023 Aug 2.
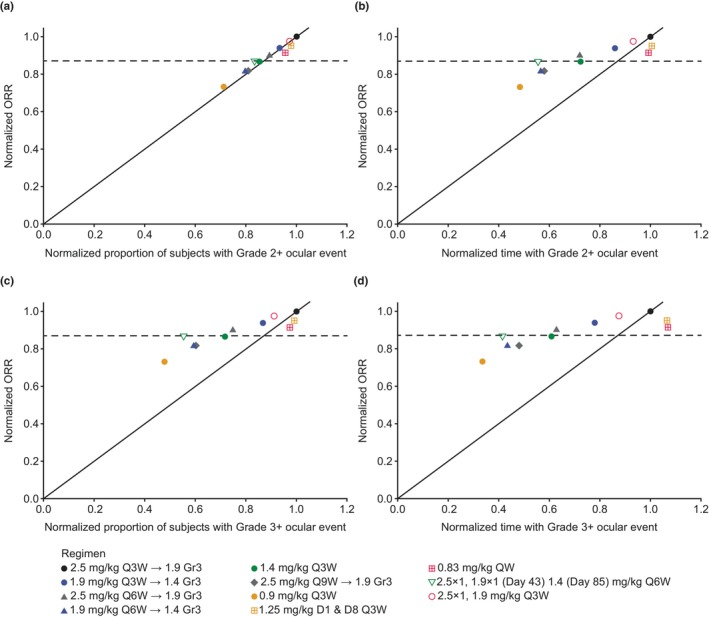
Belantamab mafodotin, a monomethyl auristatin F (MMAF)-containing monoclonal antibody-drug conjugate (ADC), demonstrated deep and durable responses in the DRiving Excellence in Approaches to Multiple Myeloma (DREAMM)-1 and pivotal DREAMM-2 studies in patients with relapsed/refractory multiple myeloma. As with other MMAF-containing ADCs, ocular adverse events were observed. To predict the effects of belantamab mafodotin dosing regimens and dose-modification strategies on efficacy and ocular safety end points, DREAMM-1 and DREAMM-2 data across a range of doses were used to develop an integrated simulation framework incorporating two separate longitudinal models and the published population pharmacokinetic model. A concentration-driven tumor growth inhibition model described the time course of serum M-protein concentration, a measure of treatment response, whereas a discrete time Markov model described the time course of ocular events graded with the GSK Keratopathy and Visual Acuity scale. Significant covariates included baseline β -microglobulin on growth rate, baseline M-protein on kill rate, extramedullary disease on the effect compartment rate constant, and baseline soluble B cell maturation antigen on maximal effect. Efficacy and safety end points were simulated for various doses with dosing intervals of 1, 3, 6, and 9 weeks and various event-driven dose-modification strategies. Simulations predicted that lower doses and longer dosing intervals were associated with lower probability and lower overall time with Grade 3+ and Grade 2+ ocular events compared with the reference regimen (2.5 mg/kg every 3 weeks), with a less-than-proportional reduction in efficacy. The predicted improved benefit-risk profiles of certain dosing schedules and dose modifications from this integrated framework has informed trial designs for belantamab mafodotin, supporting dose-optimization strategies.
贝兰他单抗马妥昔单抗,一种含有单甲基澳瑞他汀 F(MMAF)的单克隆抗体药物偶联物(ADC),在复发/难治性多发性骨髓瘤患者的 DRiving Excellence in Approaches to Multiple Myeloma(DREAMM)-1 和关键 DREAMM-2 研究中显示出深度和持久的应答。与其他含有 MMAF 的 ADC 一样,观察到了眼部不良事件。为了预测贝兰他单抗马妥昔单抗给药方案和剂量调整策略对疗效和眼部安全终点的影响,使用 DREAMM-1 和 DREAMM-2 数据在一系列剂量范围内开发了一个综合模拟框架,该框架纳入了两个独立的纵向模型和已发表的群体药代动力学模型。一个浓度驱动的肿瘤生长抑制模型描述了血清 M 蛋白浓度的时间过程,这是治疗反应的衡量标准,而一个离散时间马尔可夫模型描述了眼部事件随 GSK 角膜病和视力量表分级的时间过程。显著的协变量包括生长率的基线β-微球蛋白、杀伤率的基线 M 蛋白、效应室速率常数的髓外疾病以及最大效应的基线可溶性 B 细胞成熟抗原。用间隔 1、3、6 和 9 周的各种剂量和各种基于事件的剂量调整策略对各种剂量进行了疗效和安全性终点模拟。模拟预测,与参考方案(每 3 周 2.5mg/kg)相比,较低剂量和较长的给药间隔与 3+级和 2+级眼部事件的较低概率和总时间相关,疗效呈非比例降低。来自这个综合框架的某些给药方案和剂量修改的预测改善的获益-风险概况已为贝兰他单抗马妥昔单抗的临床试验设计提供了信息,支持剂量优化策略。