Department of Bone Marrow Transplantation, Hebei Yanda Lu Daopei Hospital, Langfang, China.
Department of Hematology, Hebei Yanda Lu Daopei Hospital, Langfang, China.
Front Immunol. 2023 Jul 4;14:1191382. doi: 10.3389/fimmu.2023.1191382. eCollection 2023.
Chimeric antigen receptor (CAR) T-cell therapy has demonstrated high initial complete remission (CR) rates in B-cell acute lymphoblastic leukemia (B-ALL) patients, including those who relapsed after transplant. However, the duration of remission requires improvements. Whether bridging to a second allogeneic hematopoietic stem cell transplant (allo-HSCT) after CAR-T therapy can improve long-term survival remains controversial. We retrospectively analyzed long-term follow-up data of B-ALL patients who relapsed post-transplant and received CAR-T therapy followed by consolidation second allo-HSCT to investigate whether such a treatment sequence could improve long-term survival.
A single-center, retrospective study was performed between October 2017 and March 2022, involving 95 patients who received a consolidation second transplant after achieving CR from CAR-T therapy.
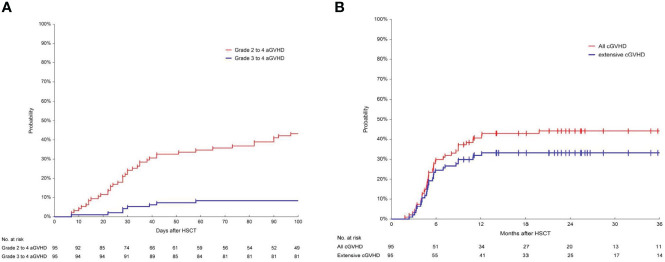
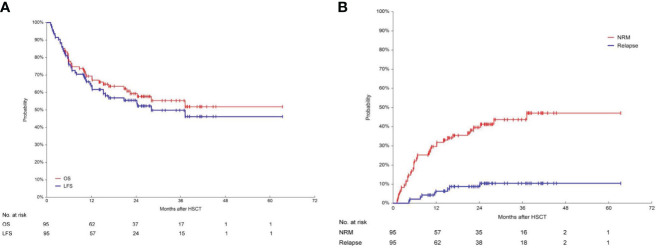
The median age of patients was 22.8 years (range: 3.3-52.8) at the second transplant. After the first transplant, 71 patients (74.7%) experienced bone marrow relapse, 16 patients (16.8%) had extramedullary relapse, 5 patients (5.3%) had both bone marrow and extramedullary relapse and 3/95 patients (3.2%) had positive minimal residual disease (MRD) only. Patients received autologous (n=57, 60.0%) or allogeneic (n=28, 29.5%) CAR-T cells, while 10 patients (10.5%) were unknown. All patients achieved CR after CAR-T therapy. Before second HSCT, 86 patients (90.5%) were MRD-negative, and 9 (9.5%) were MRD-positive. All second transplant donors were different from the first transplant donors. The median follow-up time was 623 days (range: 33-1901) after the second HSCT. The 3-year overall survival (OS) and leukemia-free survival (LFS) were 55.3% (95%CI, 44.3-66.1%) and 49.8% (95%CI, 38.7-60.9%), respectively. The 3-year relapse incidence (RI) and non-relapse mortality (NRM) were 10.5% (95%CI, 5.6-19.6%) and 43.6% (95%CI, 33.9-56.2%), respectively. In multivariate analysis, the interval from CAR-T to second HSCT ≤90 days was associated with superior LFS(HR, 4.10, 95%CI,1.64-10.24; =0.003) and OS(HR, 2.67, 95%CI, 1.24-5.74, =0.012), as well as reduced NRM (HR, 2.45, 95%CI, 1.14-5.24, =0.021).
Our study indicated that CAR-T therapy followed by consolidation second transplant could significantly improve long-term survival in B-ALL patients who relapsed post-transplant. The second transplant should be considered in suitable patients and is recommended to be performed within 90 days after CAR-T treatment.
嵌合抗原受体(CAR)T 细胞疗法在 B 细胞急性淋巴细胞白血病(B-ALL)患者中表现出高初始完全缓解(CR)率,包括那些在移植后复发的患者。然而,缓解的持续时间需要改善。CAR-T 治疗后桥接第二个异基因造血干细胞移植(allo-HSCT)是否可以改善长期生存仍存在争议。我们回顾性分析了移植后复发并接受 CAR-T 治疗后接受巩固性第二 allo-HSCT 的 B-ALL 患者的长期随访数据,以调查这种治疗顺序是否可以改善长期生存。
这是一项单中心、回顾性研究,于 2017 年 10 月至 2022 年 3 月进行,涉及 95 名在 CAR-T 治疗后达到 CR 后接受巩固性第二移植的患者。
患者在第二次移植时的中位年龄为 22.8 岁(范围:3.3-52.8)。第一次移植后,71 名患者(74.7%)出现骨髓复发,16 名患者(16.8%)出现髓外复发,5 名患者(5.3%)出现骨髓和髓外复发,3/95 名患者(3.2%)仅存在微小残留病(MRD)阳性。患者接受了自体(n=57,60.0%)或异体(n=28,29.5%)CAR-T 细胞,而 10 名患者(10.5%)未知。所有患者在 CAR-T 治疗后均达到 CR。在第二次 HSCT 之前,86 名患者(90.5%)MRD 阴性,9 名(9.5%)MRD 阳性。所有第二次移植供者均与第一次移植供者不同。第二次 HSCT 后中位随访时间为 623 天(范围:33-1901)。3 年总生存率(OS)和无白血病生存率(LFS)分别为 55.3%(95%CI,44.3-66.1%)和 49.8%(95%CI,38.7-60.9%)。3 年复发率(RI)和非复发死亡率(NRM)分别为 10.5%(95%CI,5.6-19.6%)和 43.6%(95%CI,33.9-56.2%)。多变量分析表明,CAR-T 到第二次 HSCT 的时间间隔≤90 天与更好的 LFS(HR,4.10,95%CI,1.64-10.24;=0.003)和 OS(HR,2.67,95%CI,1.24-5.74,=0.012)以及降低 NRM(HR,2.45,95%CI,1.14-5.24,=0.021)相关。
我们的研究表明,CAR-T 治疗后巩固性第二次移植可显著改善移植后复发的 B-ALL 患者的长期生存。应考虑在合适的患者中进行第二次移植,并建议在 CAR-T 治疗后 90 天内进行。