Department of Biochemistry, Assistance Publique-Hôpitaux de Paris, Paris, France.
Université Paris-Saclay, Paris, France.
Orphanet J Rare Dis. 2023 Jul 21;18(1):207. doi: 10.1186/s13023-023-02800-8.
Treatment recommendations for urea cycle disorders (UCDs) include supplementation with amino acids involved in the urea cycle (arginine and/or citrulline, depending on the enzyme deficiency), to maximize ammonia excretion through the urea cycle, but limited data are available regarding the use of citrulline. This study retrospectively reviewed clinical and biological data from patients with UCDs treated with citrulline and/or arginine at a reference center since 1990. The aim was to describe the prescription, impact, and safety of these therapies. Data collection included patient background, treatment details, changes in biochemical parameters (plasma ammonia and amino acids concentrations), decompensations, and patient outcomes.
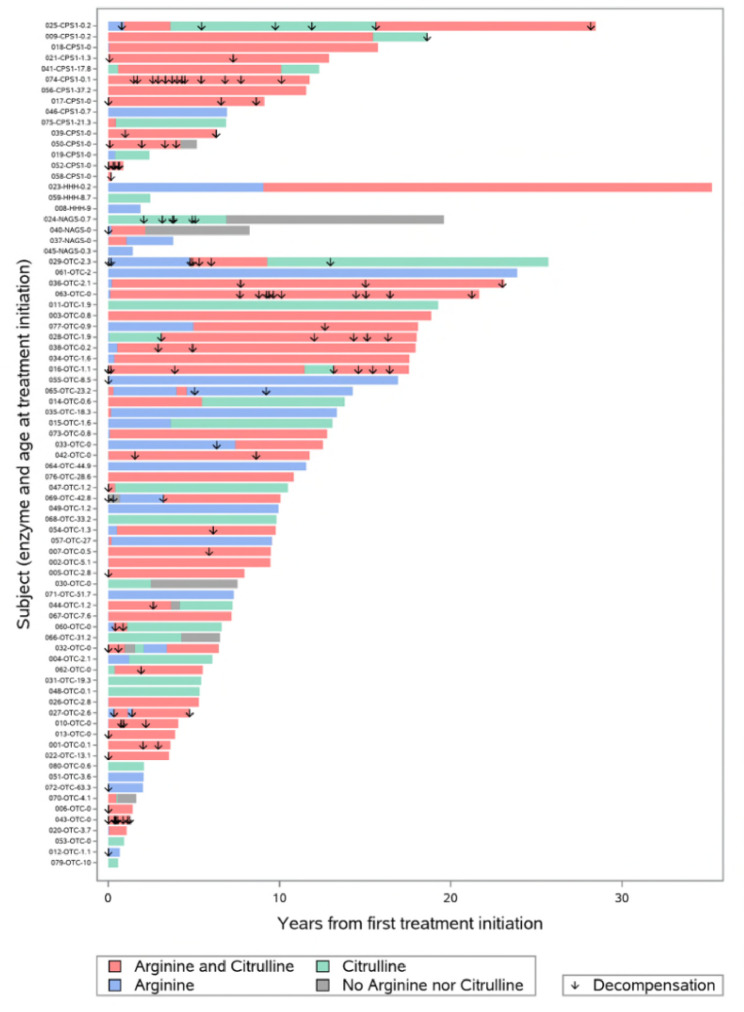
Overall, 79 patients (median age at diagnosis, 0.9 months) received citrulline and/or arginine in combination with a restricted protein diet, most with ornithine transcarbamylase (n = 57, 73%) or carbamoyl phosphate synthetase 1 (n = 15, 19%) deficiencies. Most patients also received ammonium scavengers. Median follow-up was 9.5 years and median exposure to first treatment with arginine + citrulline, citrulline monotherapy, or arginine monotherapy was 5.5, 2.5, or 0.3 years, respectively. During follow-up, arginine or citrulline was administered at least once (as monotherapy or in combination) in the same proportion of patients (86.1%); the overall median duration of exposure was 5.9 years for arginine + citrulline, 3.1 years for citrulline monotherapy, and 0.6 years for arginine monotherapy. The most common switch was from monotherapy to combination therapy (41 of 75 switches, 54.7%). During treatment, mean ammonia concentrations were 35.9 µmol/L with citrulline, 49.8 µmol/L with arginine, and 53.0 µmol/L with arginine + citrulline. Mean plasma arginine concentrations increased significantly from the beginning to the end of citrulline treatment periods (from 67.6 µmol/L to 84.9 µmol/L, P < 0.05). At last evaluation, mean height and weight for age were normal and most patients showed normal or adapted behavior (98.7%) and normal social life (79.0%). Two patients (2.5%) experienced three treatment-related gastrointestinal adverse reactions.
This study underlines the importance of citrulline supplementation, either alone or together with arginine, in the management of patients with UCDs. When a monotherapy is considered, citrulline would be the preferred option in terms of increasing plasma arginine concentrations.
尿素循环障碍(UCD)的治疗建议包括补充参与尿素循环的氨基酸(精氨酸和/或瓜氨酸,取决于酶缺乏情况),以通过尿素循环最大限度地排泄氨,但关于瓜氨酸的使用,数据有限。本研究回顾性分析了自 1990 年以来在参考中心接受瓜氨酸和/或精氨酸治疗的 UCD 患者的临床和生物学数据。目的是描述这些治疗的处方、影响和安全性。数据收集包括患者背景、治疗细节、生化参数(血浆氨和氨基酸浓度)变化、失代偿和患者结局。
总体而言,79 名患者(中位诊断年龄 0.9 个月)接受了瓜氨酸和/或精氨酸联合限制蛋白饮食治疗,其中大多数为鸟氨酸转氨甲酰酶(n=57,73%)或氨甲酰磷酸合成酶 1(n=15,19%)缺乏症。大多数患者还接受了氨清除剂治疗。中位随访时间为 9.5 年,首次接受精氨酸+瓜氨酸、瓜氨酸单药或精氨酸单药治疗的中位暴露时间分别为 5.5、2.5 和 0.3 年。在随访期间,86.1%的患者至少一次(单药或联合)接受了精氨酸或瓜氨酸治疗;精氨酸+瓜氨酸的总体中位暴露时间为 5.9 年,瓜氨酸单药治疗为 3.1 年,精氨酸单药治疗为 0.6 年。最常见的转换是从单药治疗转换为联合治疗(41 次转换中的 41 次,54.7%)。治疗期间,瓜氨酸组的平均氨浓度为 35.9µmol/L,精氨酸组为 49.8µmol/L,精氨酸+瓜氨酸组为 53.0µmol/L。瓜氨酸治疗期间,血浆精氨酸浓度从开始到结束显著升高(从 67.6µmol/L 增加到 84.9µmol/L,P<0.05)。最后评估时,身高和体重的年龄均正常,大多数患者表现出正常或适应行为(98.7%)和正常社交生活(79.0%)。两名患者(2.5%)经历了三种与治疗相关的胃肠道不良反应。
本研究强调了在 UCD 患者管理中补充瓜氨酸的重要性,无论是单独使用还是与精氨酸联合使用。在考虑单药治疗时,瓜氨酸在增加血浆精氨酸浓度方面是首选。