Pharmacoepidemiology and Drug Safety Research Group, Department of Pharmacy, Faculty of Mathematics and Natural Sciences, University of Oslo, Oslo, Norway.
Faculty of Medicine, Institute for Health and Society, University of Oslo, Oslo, Norway.
Arch Womens Ment Health. 2023 Oct;26(5):669-683. doi: 10.1007/s00737-023-01341-0. Epub 2023 Jul 22.
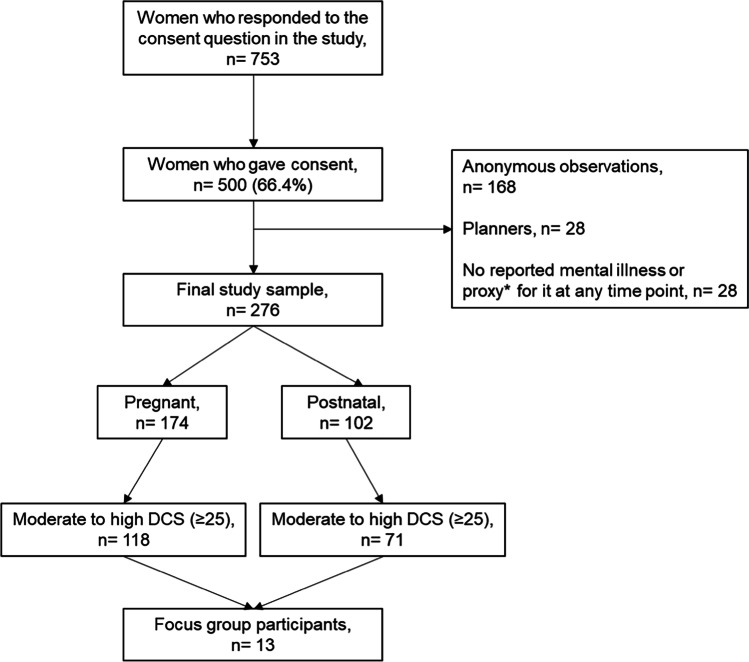
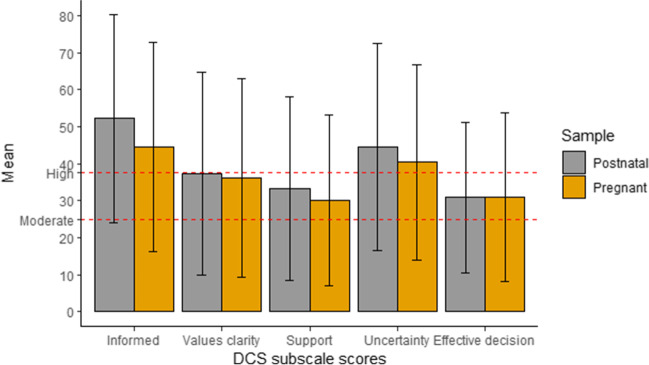
This study aims to investigate decisional conflict and elucidate challenges in decision-making among perinatal women using or considering using antidepressant (AD) during pregnancy. A sequential, mixed-methods study was employed among pregnant and postnatal women in Norway who had been offered ADs in the last 5 years. Quantitative data were obtained through an electronic questionnaire. Decisional conflict in pregnancy was assessed using the Decisional Conflict Scale (DCS) defined as either low (< 25) or moderate-high ( ≥ 25) (evaluated retrospectively for postnatal women). Logistic regression was used to identify factors associated with moderate-high decisional conflict. Qualitative data were collected through focus groups with pregnant and postnatal women, and an inductive approach was used for data analysis. Among 174 pregnant and 102 postnatal women, 67.8% and 69.6%, respectively, reported moderate-high decisional conflict during pregnancy. Unsatisfactory doctor-patient relationship was associated with greater likelihood of having moderate-high decisional conflict in pregnancy, both in pregnant (aOR = 1.20, 95% CI: 1.00-1.44) and postnatal women (aOR = 1.40, 95% CI: 1.08-1.82). Reported barriers to decision-making regarding AD use in pregnancy encompassed five DCS subscales: uninformed knowledge following contradictory research and unfamiliarity with authorised resources, unclear values due to emotional blunting and fear associated with AD use, inadequate support, uncertainty in decisions and ineffective decisions due to difficulty in finding personalised treatment, and diverging recommendations by the healthcare providers (HCPs). The quality of the interaction with the HCP plays a crucial role in managing decisional conflict and supporting informed decisions in the management of perinatal mental illness. This study highlights the need for increased provision of clear, evidence-based information by HCPs to facilitate shared decision-making and create personalised treatments for perinatal women considering AD use during pregnancy.
本研究旨在调查围产期女性在使用或考虑使用抗抑郁药(AD)时的决策冲突,并阐明决策过程中的挑战。该研究采用序贯混合方法,在挪威对过去 5 年内接受过 AD 治疗的孕妇和产后女性进行了研究。通过电子问卷获得定量数据。使用决策冲突量表(DCS)评估妊娠期的决策冲突,将其定义为低(<25)或中高(≥25)(对产后女性进行回顾性评估)。采用逻辑回归识别与中高决策冲突相关的因素。通过对孕妇和产后女性的焦点小组收集定性数据,并采用归纳法进行数据分析。在 174 名孕妇和 102 名产后女性中,分别有 67.8%和 69.6%的人报告在怀孕期间存在中高决策冲突。不满意的医患关系与孕妇(优势比 [OR] = 1.20,95%置信区间:1.00-1.44)和产后女性(OR = 1.40,95%置信区间:1.08-1.82)中更有可能出现中高决策冲突有关。与怀孕期间使用 AD 相关的决策障碍包括五个 DCS 子量表:研究结果相互矛盾且缺乏授权资源,导致知识匮乏;情绪迟钝和对 AD 使用的恐惧导致价值观不明确;支持不足;因难以找到个性化治疗而导致决策不确定和决策无效;以及医疗保健提供者(HCP)的建议存在差异。与 HCP 的互动质量在管理决策冲突和支持围产期精神疾病管理中的知情决策方面发挥着至关重要的作用。本研究强调 HCP 需要增加提供清晰、基于证据的信息,以促进共同决策并为考虑在怀孕期间使用 AD 的围产期女性制定个性化治疗方案。