Khoiwal Kavita, Sheoran Deepika, Mishra Ramya, Gaurav Amrita, Chaturvedi Jaya
Dept. of Obstetrics & Gynaecology, AIIMS, Rishikesh, Uttarakhand, India.
Eur J Obstet Gynecol Reprod Biol X. 2023 Jul 5;19:100212. doi: 10.1016/j.eurox.2023.100212. eCollection 2023 Sep.
To ascertain whether extra-peritoneal approach is superior to conventional trans-peritoneal approach of cesarean section in terms of fetus delivery time, intra-operative and postoperative outcomes, including return of bowel activity and pain.
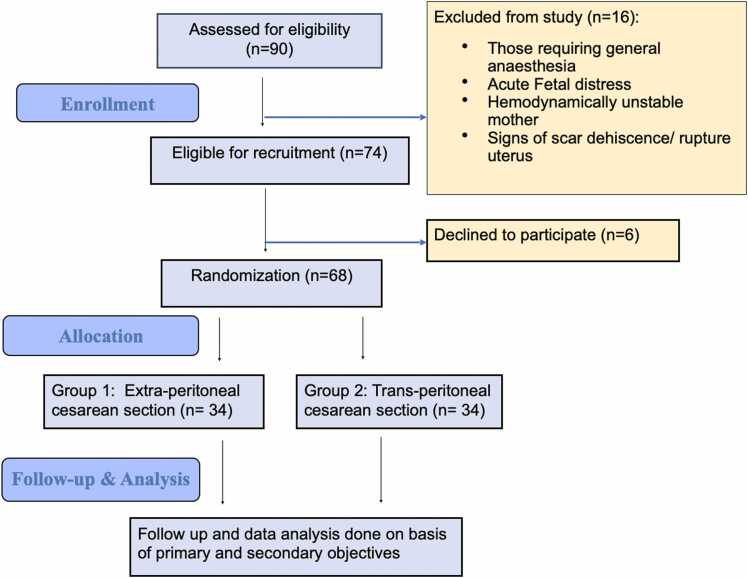
An open-label randomized controlled trial conducted over one year and six months at a tertiary care center in India. As per sample size calculation, 68 women enrolled in the study; 34 underwent extra-peritoneal, and another 34 underwent trans-peritoneal cesarean section after randomization. Statistical analysis was done with independent sample 't' test, chi-squared test, and fisher's exact test.
Baseline characteristics were comparable in both groups. Fetus delivery time was significantly higher in extra-peritoneal than trans-peritoneal cesarean section (14.26 ± 1.26 vs. 9.38 ± 1.83 min; p = <0.001). Total operation time was also higher in extra-peritoneal than trans-peritoneal approach (63.24 ± 12.74 vs. 57.41 ± 8.62 min; p = 0.027). Whereas average blood loss was comparable in both groups (733.82 ± 219.06 vs. 694.12 ± 351.57 ml; p = 0.063). Postoperatively, return of bowel activity was significantly earlier in extra-peritoneal than trans-peritoneal approach (4.59 ± 0.56 vs. 8.65 ± 1.23 h; p = <0.001). Mean time taken for passage of flatus was also significantly less in extra-peritoneal cesarean section (8.56 ± 0.99 vs. 12.76 ± 2.05 h; p = <0.001). Pain score at 6, 12, and 18 h was significantly lower in extra-peritoneal approach. No patient in extra-peritoneal approach had nausea, vomiting, and abdominal distension. Whereas 11.8 % of patients had nausea, 5.9 % had constipation, and 14.7 % had abdominal distension in trans-peritoneal cesarean section. Requirement of injectable antibiotics and analgesics, and hospital stay was less with extra-peritoneal approach.
Extra-peritoneal cesarean section is associated with better postoperative outcomes with respect to return of bowel functions, pain, and requirement of injectable analgesics and antibiotics than the routine trans-peritoneal cesarean section. However, the significantly higher fetus delivery time questions its feasibility in patients with acute fetal distress. Additionally, it is technically difficult and has a longer learning curve.
确定在胎儿娩出时间、术中及术后结局(包括肠道功能恢复和疼痛情况)方面,剖宫产的腹膜外途径是否优于传统的经腹途径。
在印度一家三级医疗中心进行的一项为期一年零六个月的开放标签随机对照试验。根据样本量计算,68名女性纳入研究;随机分组后,34例行腹膜外剖宫产,另外34例行经腹剖宫产。采用独立样本t检验、卡方检验和Fisher精确检验进行统计分析。
两组的基线特征具有可比性。腹膜外剖宫产的胎儿娩出时间显著长于经腹剖宫产(14.26±1.26分钟 vs. 9.38±1.83分钟;p =<0.001)。腹膜外途径的总手术时间也长于经腹途径(63.24±12.74分钟 vs. 57.41±8.62分钟;p = 0.027)。而两组的平均失血量具有可比性(733.82±219.06毫升 vs. 694.12±351.57毫升;p = 0.063)。术后,腹膜外途径的肠道功能恢复明显早于经腹途径(4.59±0.56小时 vs. 8.65±1.23小时;p =<0.001)。腹膜外剖宫产排气的平均时间也显著缩短(8.56±0.99小时 vs. 12.76±2.05小时;p =<0.001)。腹膜外途径在6小时、12小时和18小时的疼痛评分显著更低。腹膜外途径组无患者出现恶心、呕吐和腹胀。而经腹剖宫产组有11.8%的患者出现恶心,5.9%的患者出现便秘,14.7%的患者出现腹胀。腹膜外途径使用注射用抗生素和镇痛药的需求以及住院时间更少。
与常规经腹剖宫产相比,腹膜外剖宫产在肠道功能恢复、疼痛以及注射用镇痛药和抗生素的需求方面具有更好的术后结局。然而,胎儿娩出时间显著更长,这对其在急性胎儿窘迫患者中的可行性提出了质疑。此外,该方法技术难度大,学习曲线较长。