Kim Tae Hyun, Kim Bo Hyun, Cho Yu Ri, Koh Young-Hwan, Park Joong-Won
Center for Liver and Pancreatobiliary Cancer, National Cancer Center, Goyang, Korea.
Proton Therapy Center, National Cancer Center, Goyang, Korea.
J Liver Cancer. 2023 Sep;23(2):330-340. doi: 10.17998/jlc.2023.04.14. Epub 2023 May 16.
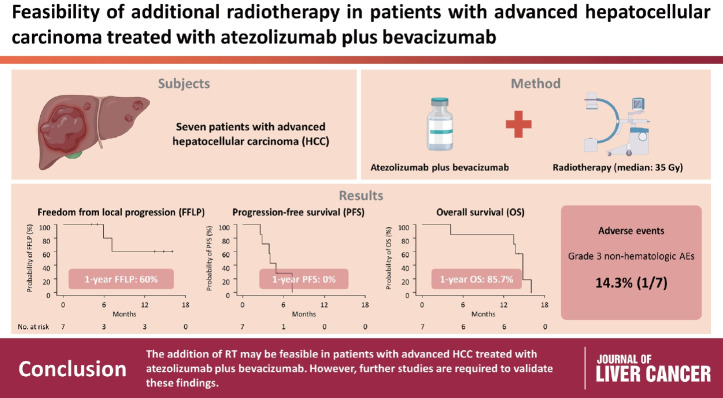
BACKGROUND/AIM: Radiotherapy (RT) is an effective local treatment for hepatocellular carcinoma (HCC). However, whether additional RT is safe and effective in patients with advanced HCC receiving atezolizumab plus bevacizumab remains unclear. This retrospective cohort study aimed to evaluate the feasibility of additional RT in these patients.
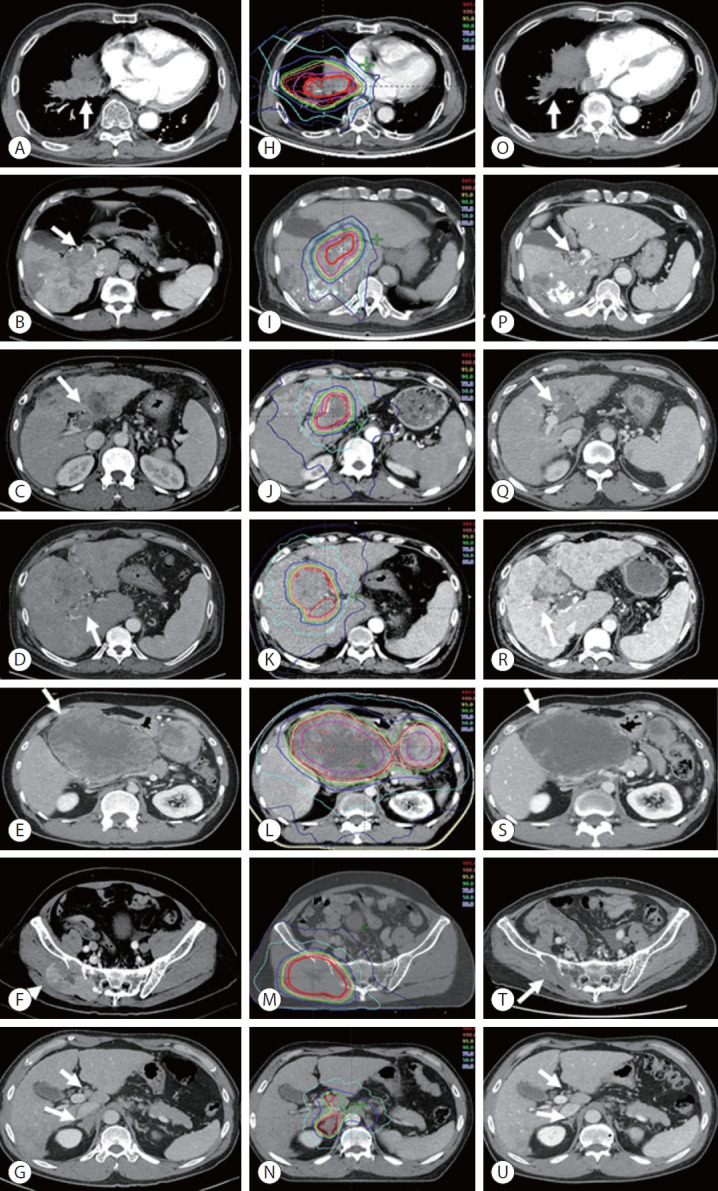
Between March and October 2021, we retrospectively analyzed seven patients with advanced HCC who received RT during treatment with atezolizumab plus bevacizumab. The median prescribed RT dose was 35 Gy (range, 33-66). Freedom from local progression (FFLP), progression-free survival (PFS), and overall survival (OS) after RT were analyzed.
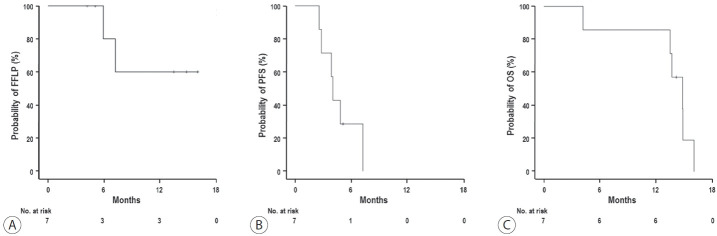
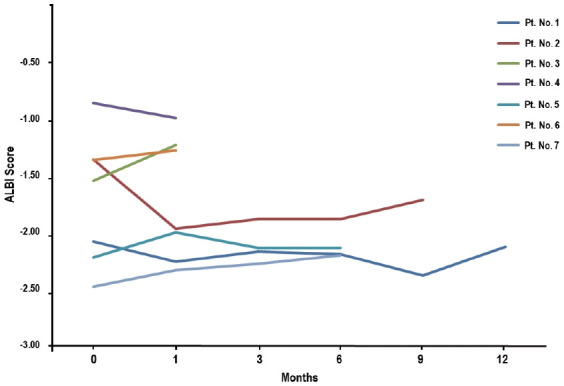
The median follow-up duration after RT was 14.2 months (range, 10.0-18.6). Of the seven patients, disease progression was noted in six (85.7%), the sites of disease progression were local in two (28.6%), intrahepatic in four (57.1%), and extrahepatic in four (57.1%). The median time of FFLP was not reached, and PFS and OS times were 4.0 (95% confidence interval [CI], 3.6-4.5) and 14.8% (95% CI, 12.5-17.2) months, respectively. The 1-year FFLP, PFS, and OS rates were 60% (95% CI, 43.8-76.2), 0%, and 85.7% (95% CI, 75.9-95.5), respectively. Grade 3 or higher hematologic adverse events (AEs) were not observed, but grade 3 nonhematologic AEs unrelated to RT were observed in one patient.
The addition of RT may be feasible in patients with advanced HCC treated with atezolizumab plus bevacizumab. However, further studies are required to validate these findings.
背景/目的:放射治疗(RT)是肝细胞癌(HCC)的一种有效局部治疗方法。然而,对于接受阿替利珠单抗联合贝伐单抗治疗的晚期HCC患者,额外进行RT是否安全有效仍不清楚。这项回顾性队列研究旨在评估在这些患者中额外进行RT的可行性。
2021年3月至10月期间,我们回顾性分析了7例在接受阿替利珠单抗联合贝伐单抗治疗期间接受RT的晚期HCC患者。规定的RT中位剂量为35 Gy(范围33 - 66)。分析了RT后的无局部进展生存期(FFLP)、无进展生存期(PFS)和总生存期(OS)。
RT后的中位随访时间为14.2个月(范围10.0 - 18.6)。7例患者中,6例(85.7%)出现疾病进展,疾病进展部位为局部的2例(28.6%),肝内的4例(57.1%),肝外的4例(57.1%)。未达到FFLP的中位时间,PFS和OS时间分别为4.0(95%置信区间[CI],3.6 - 4.5)个月和14.8%(95% CI,12.5 - 17.2)个月。1年FFLP、PFS和OS率分别为60%(95% CI,43.8 - 76.2)、0%和85.7%(95% CI,75.9 - 95.5)。未观察到3级或更高等级的血液学不良事件(AE),但1例患者观察到与RT无关的3级非血液学AE。
对于接受阿替利珠单抗联合贝伐单抗治疗的晚期HCC患者,额外进行RT可能是可行的。然而,需要进一步研究来验证这些发现。