Division of Medicine, University College London Centre for Obesity Research, Rayne Institute, London, United Kingdom.
Bariatric Centre for Weight Management and Metabolic Surgery, University College London Hospitals, National Health Service Foundation Trust, London, United Kingdom.
JAMA Surg. 2023 Oct 1;158(10):1003-1011. doi: 10.1001/jamasurg.2023.2930.
Metabolic surgery leads to weight loss and improved health, but these outcomes are highly variable. Poor weight loss is associated with lower circulating levels of glucagon-like peptide-1 (GLP-1).
To assess the efficacy and safety of the GLP-1 receptor agonist, liraglutide, 3.0 mg, on percentage body weight reduction in patients with poor weight loss and suboptimal GLP-1 response after metabolic surgery.
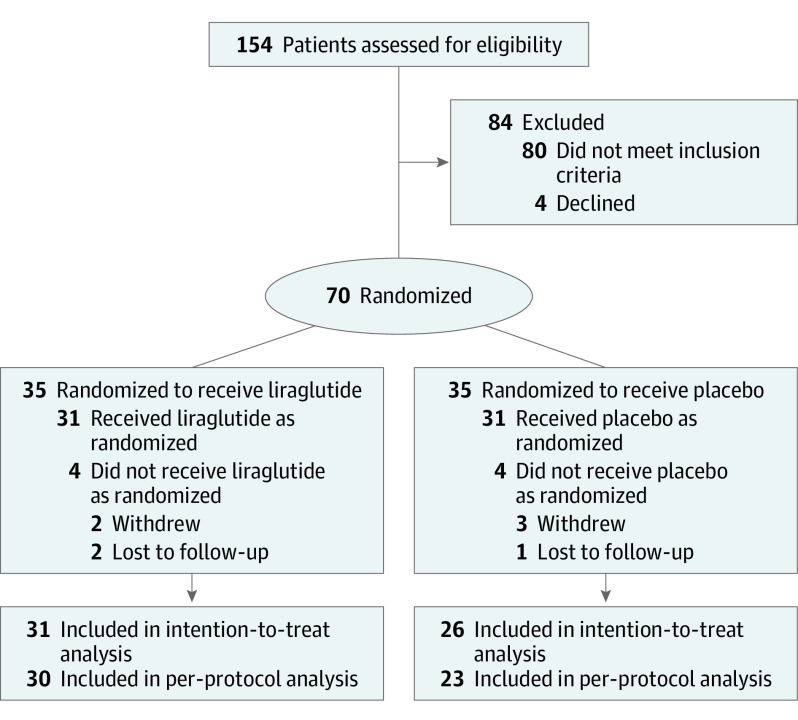
DESIGN, SETTING, AND PARTICIPANTS: The Evaluation of Liraglutide 3.0 mg in Patients With Poor Weight Loss and a Suboptimal Glucagon-Like Peptide-1 Response (BARI-OPTIMISE) randomized placebo-controlled trial recruited adult patients at least 1 year after metabolic surgery who had experienced 20% or less body weight loss from the day of surgery and a suboptimal nutrient-stimulated GLP-1 response from 2 hospitals in London, United Kingdom, between October 2018 and November 2019. Key exclusion criteria were type 1 diabetes; severe concomitant psychiatric, gastrointestinal, cardiac, kidney or metabolic disease; and use of insulin, GLP-1 receptor analogues, and medication that can affect weight. The study period was 24 weeks followed by a 4-week follow-up period. Last participant follow-up was completed in June 2020. All participants and clinical study personnel were blinded to treatment allocation. Of 154 assessed for eligibility, 70 met trial criteria and were included in the study, and 57 completed follow-up.
Liraglutide, 3.0 mg, once daily or placebo as an adjunct to lifestyle intervention with a 500-kcal daily energy deficit for 24 weeks, on a 1:1 allocation by computer-generated randomization sequence, stratified by surgery type (Roux-en-Y gastric bypass [RYGB] or sleeve gastrectomy [SG]) and type 2 diabetes status.
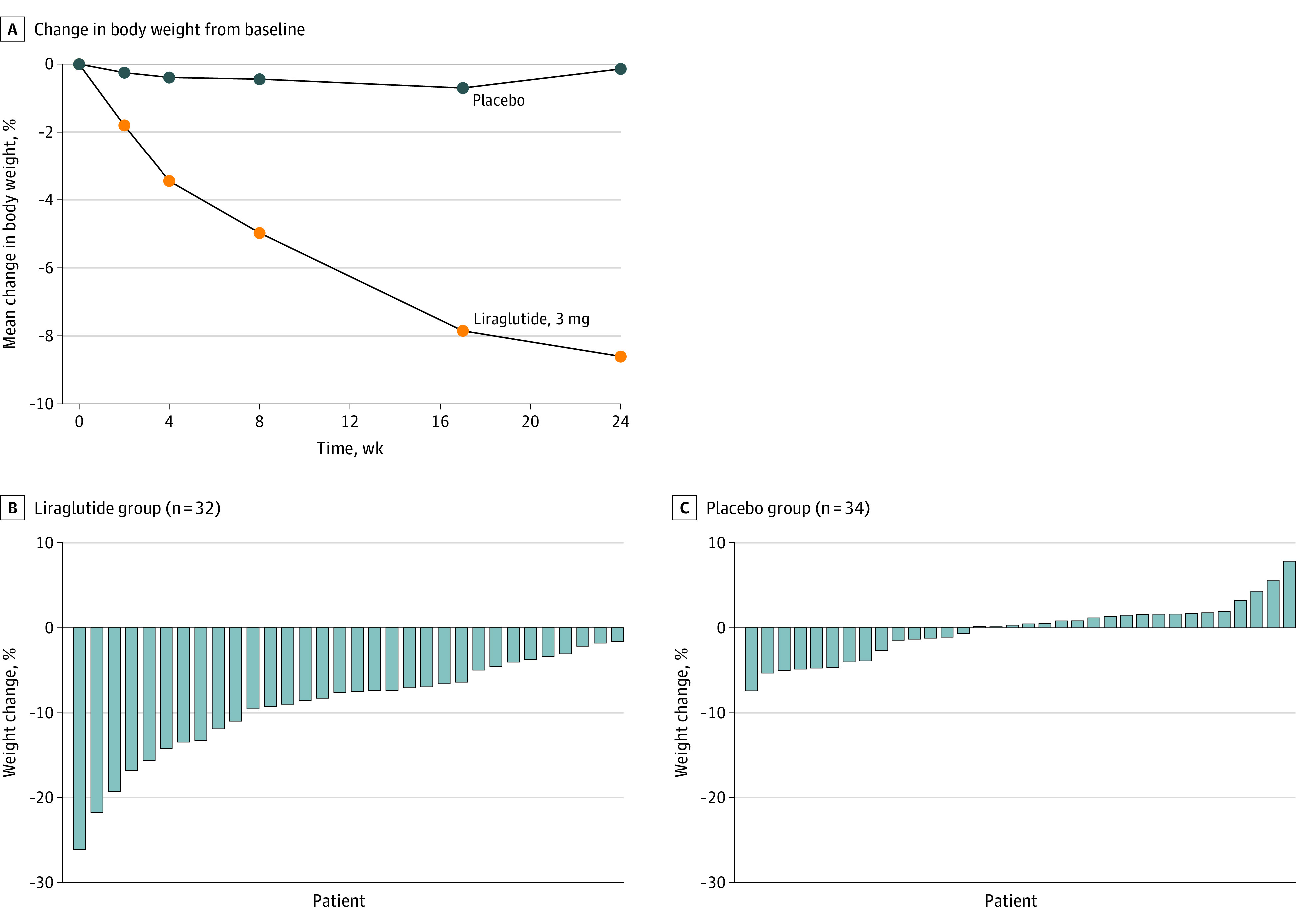
The primary outcome was change in percentage body weight from baseline to the end of the 24-week study period based on an intention-to-treat analysis. Participant safety was assessed through monitoring of biochemical parameters, including kidney and liver function, physical examination, and assessment for adverse events.
A total of 70 participants (mean [SD] age, 47.6 [10.7] years; 52 [74%] female) with a poor weight loss response following RYGB or SG were randomized to receive 3.0-mg liraglutide (n = 35) or placebo (n = 35). All participants received at least 1 dose of the trial drug. Eight participants discontinued treatment (4 per group), and 2 in the 3.0-mg liraglutide group and 1 in the placebo group were lost to follow-up. Due to COVID-19 restrictions, 3 participants in the 3.0-mg liraglutide group and 7 in the placebo group were unable to attend their final in-person assessment. Estimated change in mean (SD) percentage body weight from baseline to week 24 was -8.82 (4.94) with liraglutide, 3.0 mg (n = 31), vs -0.54 (3.32) with placebo (n = 26). The mean difference in percentage body weight change for liraglutide, 3.0 mg, vs placebo was -8.03 (95% CI, -10.39 to -5.66; P < .001). Adverse events, predominantly gastrointestinal, were more frequent with liraglutide, 3.0 mg (28 events [80%]), than placebo (20 events [57%]). There were no serious adverse events and no treatment-related deaths.
These findings support the use of adjuvant liraglutide, 3.0 mg, for weight management in patients with poor weight loss and suboptimal GLP-1 response after metabolic surgery.
ClinicalTrials.gov Identifier: NCT03341429.
重要性:代谢手术可导致体重减轻和健康状况改善,但这些结果的个体差异很大。体重减轻不佳与循环中胰高血糖素样肽-1(GLP-1)水平降低有关。
目的:评估 GLP-1 受体激动剂利拉鲁肽 3.0mg 对代谢手术后体重减轻不佳和 GLP-1 反应不佳的患者的体重百分比降低的疗效和安全性。
设计、地点和参与者:代谢手术后体重减轻不佳且 GLP-1 反应不佳的患者中利拉鲁肽 3.0mg 的评估(BARI-OPTIMISE)是一项随机、安慰剂对照试验,招募了至少在英国伦敦的 2 家医院进行代谢手术后 1 年以上、术后体重减轻 20%或以下且营养刺激后 GLP-1 反应不佳的成年患者。主要排除标准为 1 型糖尿病;严重合并的精神、胃肠道、心脏、肾脏或代谢疾病;以及使用胰岛素、GLP-1 受体类似物和可能影响体重的药物。研究期为 24 周,随后进行 4 周的随访期。最后一次随访于 2020 年 6 月完成。所有参与者和临床研究人员均对治疗分配进行了盲法。在评估的 154 名合格患者中,有 70 名符合试验标准并被纳入研究,其中 57 名完成了随访。
干预措施:利拉鲁肽 3.0mg 每日一次或安慰剂作为生活方式干预的辅助治疗,24 周内每日能量摄入减少 500 卡路里,采用计算机生成的随机序列以 1:1 的比例分配,按手术类型(Roux-en-Y 胃旁路术[RYGB]或袖状胃切除术[SG])和 2 型糖尿病状态分层。
主要结果和措施:主要结局是基于意向治疗分析,从基线到 24 周研究结束时的体重百分比变化。通过监测生化参数(包括肾功能和肝功能、体格检查和不良事件评估)来评估参与者的安全性。
结果:共有 70 名(平均[标准差]年龄,47.6[10.7]岁;52[74%]女性)在 RYGB 或 SG 后出现体重减轻反应不佳的患者被随机分配接受 3.0mg 利拉鲁肽(n=35)或安慰剂(n=35)。所有参与者至少接受了 1 次试验药物治疗。8 名参与者停止治疗(每组 4 名),2 名利拉鲁肽组和 1 名利拉鲁肽组的参与者失访。由于 COVID-19 限制,3 名利拉鲁肽组和 7 名利拉鲁肽组的参与者无法参加他们的最后一次现场评估。估计从基线到第 24 周的平均(SD)体重百分比变化为利拉鲁肽 3.0mg(n=31)为-8.82(4.94),安慰剂(n=26)为-0.54(3.32)。利拉鲁肽 3.0mg 与安慰剂相比,体重百分比变化的平均差异为-8.03(95%CI,-10.39 至-5.66;P<0.001)。利拉鲁肽 3.0mg(28 例[80%])的不良事件,主要为胃肠道,比安慰剂(20 例[57%])更频繁。没有严重不良事件和与治疗相关的死亡。
结论和相关性:这些发现支持在代谢手术后体重减轻不佳和 GLP-1 反应不佳的患者中使用辅助利拉鲁肽 3.0mg 进行体重管理。
试验注册:ClinicalTrials.gov 标识符:NCT03341429。