Multidisciplinary Cardiovascular Research Centre & Department of Biomedical Imaging Science, Leeds Institute of Cardiovascular and Metabolic Medicine, University of Leeds, Leeds, LS2 9JT, UK.
Department of Cardiology, Wythenshawe Hospital, Manchester University NHS Trust, Manchester, UK.
J Cardiovasc Magn Reson. 2023 Jul 27;25(1):43. doi: 10.1186/s12968-023-00946-9.
When feasible, guidelines recommend mitral valve repair (MVr) over mitral valve replacement (MVR) to treat primary mitral regurgitation (MR), based upon historic outcome studies and transthoracic echocardiography (TTE) reverse remodeling studies. Cardiovascular magnetic resonance (CMR) offers reference standard biventricular assessment with superior MR quantification compared to TTE. Using serial CMR in primary MR patients, we aimed to investigate cardiac reverse remodeling and residual MR post-MVr vs MVR with chordal preservation.
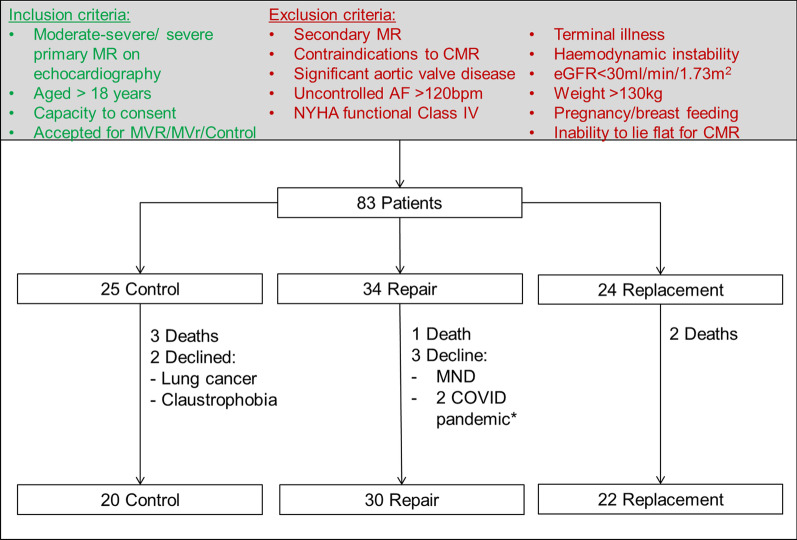
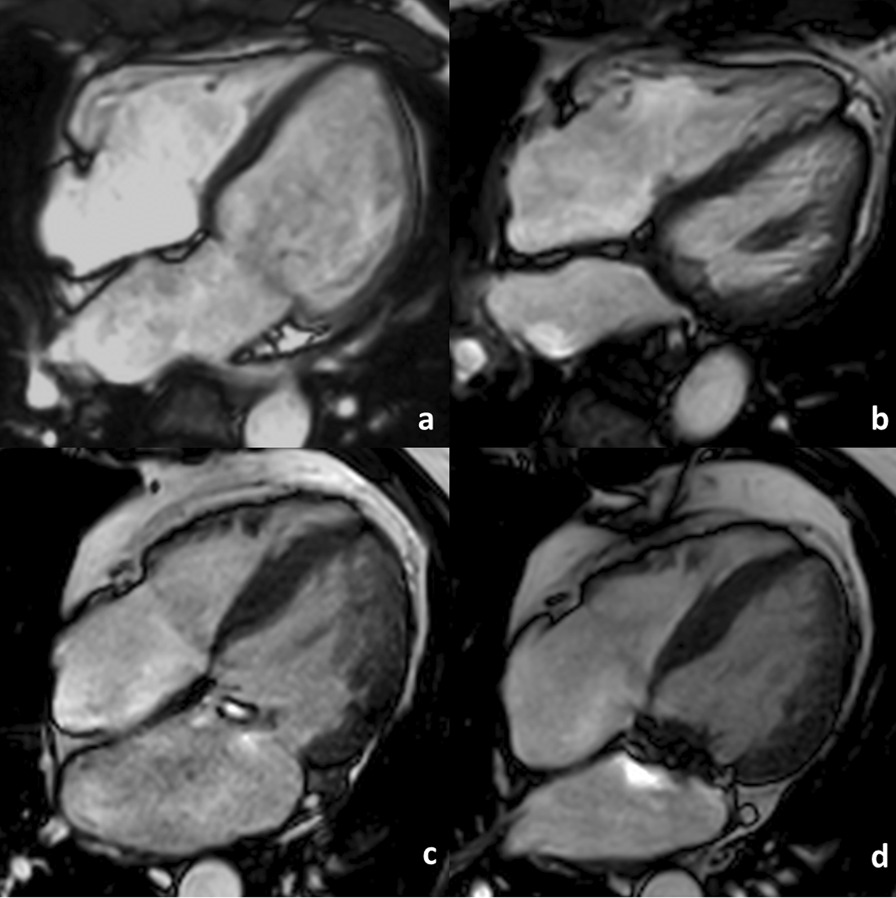
83 patients with ≥ moderate-severe MR on TTE were prospectively recruited. 6-min walk tests (6MWT) and CMR imaging including cine imaging, aortic/pulmonary through-plane phase contrast imaging, T1 maps and late-gadolinium-enhanced (LGE) imaging were performed at baseline and 6 months after mitral surgery or watchful waiting (control group).
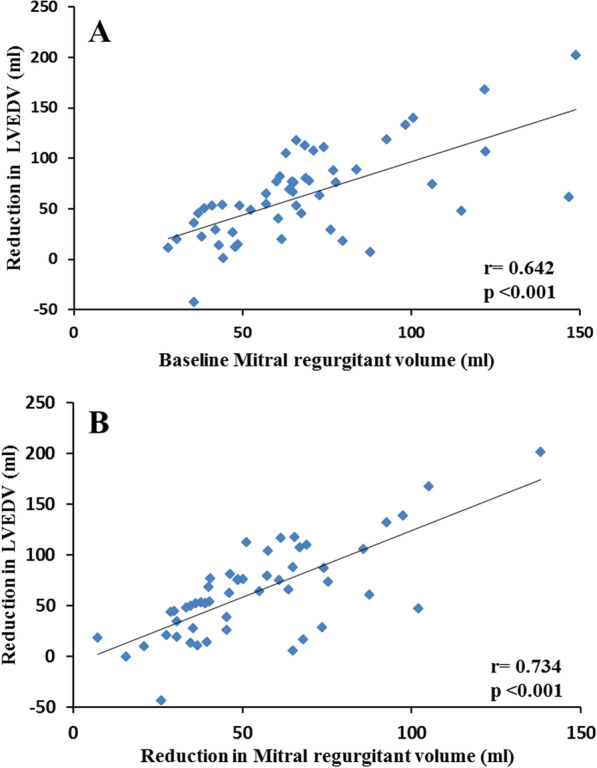
72 patients completed follow-up (Controls = 20, MVr = 30 and MVR = 22). Surgical groups demonstrated comparable baseline cardiac indices and co-morbidities. At 6-months, MVr and MVR groups demonstrated comparable improvements in 6MWT distances (+ 57 ± 54 m vs + 64 ± 76 m respectively, p = 1), reduced indexed left ventricular end-diastolic volumes (LVEDVi; - 29 ± 21 ml/m vs - 37 ± 22 ml/m respectively, p = 0.584) and left atrial volumes (- 23 ± 30 ml/m and - 39 ± 26 ml/m respectively, p = 0.545). At 6-months, compared with controls, right ventricular ejection fraction was poorer post-MVr (47 ± 6.1% vs 53 ± 8.0% respectively, p = 0.01) compared to post-MVR (50 ± 5.7% vs 53 ± 8.0% respectively, p = 0.698). MVR resulted in lower residual MR-regurgitant fraction (RF) than MVr (12 ± 8.0% vs 21 ± 11% respectively, p = 0.022). Baseline and follow-up indices of diffuse and focal myocardial fibrosis (Native T1 relaxation times, extra-cellular volume and quantified LGE respectively) were comparable between groups. Stepwise multiple linear regression of indexed variables in the surgical groups demonstrated baseline indexed mitral regurgitant volume as the sole multivariate predictor of left ventricular (LV) end-diastolic reverse remodelling, baseline LVEDVi as the most significant independent multivariate predictor of follow-up LVEDVi, baseline indexed LV end-systolic volume as the sole multivariate predictor of follow-up LV ejection fraction and undergoing MVR (vs MVr) as the most significant (p < 0.001) baseline multivariate predictor of lower residual MR.
In primary MR, MVR with chordal preservation may offer comparable cardiac reverse remodeling and functional benefits at 6-months when compared to MVr. Larger, multicenter CMR studies are required, which if the findings are confirmed could impact future surgical practice.
基于历史结果研究和经胸超声心动图(TTE)逆向重构研究,指南建议在可行的情况下,对于原发性二尖瓣反流(MR)患者,采用二尖瓣修复术(MVr)而非二尖瓣置换术(MVR),因为前者的效果优于后者。心血管磁共振(CMR)提供了参考标准的双心室评估,并能更好地定量 MR。本研究旨在通过原发性 MR 患者的连续 CMR,研究 MVr 与保留腱索的 MVR 术后的心脏逆向重构和残余 MR。
前瞻性纳入了 83 例 TTE 检查提示中重度以上 MR 的患者。所有患者均进行了 6 分钟步行测试(6MWT)和 CMR 成像检查,包括电影成像、主动脉/肺动脉平面内相位对比成像、T1 图谱和晚期钆增强(LGE)成像。这些检查分别在基线时和二尖瓣手术后或密切观察(对照组)的 6 个月时进行。
72 例患者完成了随访(对照组 20 例,MVr 组 30 例,MVR 组 22 例)。手术组患者具有相似的基线心脏指数和合并症。6 个月时,MVr 组和 MVR 组的 6MWT 距离均有相似的改善(分别增加了+57±54 m 和+64±76 m,p=1),左心室舒张末期容积指数(LVEDVi)减少(分别减少了-29±21 ml/m 和-37±22 ml/m,p=0.584)和左心房容积减少(分别减少了-23±30 ml/m 和-39±26 ml/m,p=0.545)。6 个月时,与对照组相比,MVr 组的右心室射血分数较差(分别为 47±6.1%和 53±8.0%,p=0.01),而 MVR 组的右心室射血分数与对照组相似(分别为 50±5.7%和 53±8.0%,p=0.698)。MVR 组的残余 MR 反流分数(RF)明显低于 MVr 组(分别为 12±8.0%和 21±11%,p=0.022)。各组之间的弥漫性和局灶性心肌纤维化的基线和随访指数(分别为 Native T1 弛豫时间、细胞外体积和定量 LGE)均无差异。手术组的指数变量逐步多元线性回归显示,基线指数二尖瓣反流容积是左心室(LV)舒张末期逆向重构的唯一多变量预测因素,基线 LVEDVi 是随访 LVEDVi 的最显著的独立多变量预测因素,基线指数 LV 收缩末期容积是随访 LV 射血分数的唯一多变量预测因素,而接受 MVR(而非 MVr)是残余 MR 最低的最显著的(p<0.001)多变量预测因素。
在原发性 MR 中,与 MVr 相比,保留腱索的 MVR 在 6 个月时可能具有相似的心脏逆向重构和功能获益。需要进行更大规模的多中心 CMR 研究,如果这些发现得到证实,可能会影响未来的手术实践。