Verspoor Floortje G M, Hannink Gerjon, Parry Michael, Jeys Lee, Stevenson Jonathan D
Department of Oncology, Royal Orthopaedic Hospital, Birmingham, UK.
Amsterdam UMC, Department of Orthopaedic Surgery, University of Amsterdam, Amsterdam Movement Sciences, Amsterdam, The Netherlands.
Ann Surg Oncol. 2023 Nov;30(12):7882-7891. doi: 10.1245/s10434-023-13931-4. Epub 2023 Jul 28.
The optimal surgical treatment for patients presenting with (impending and complete) pathological proximal femoral fractures is predicated on prognosis. Guidelines recommend a preoperative biopsy to exclude sarcomas, however no evidence confirms a benefit.
This study aimed to describe the diagnostic accuracy, morbidity and sarcoma incidence of biopsy results in these patients.
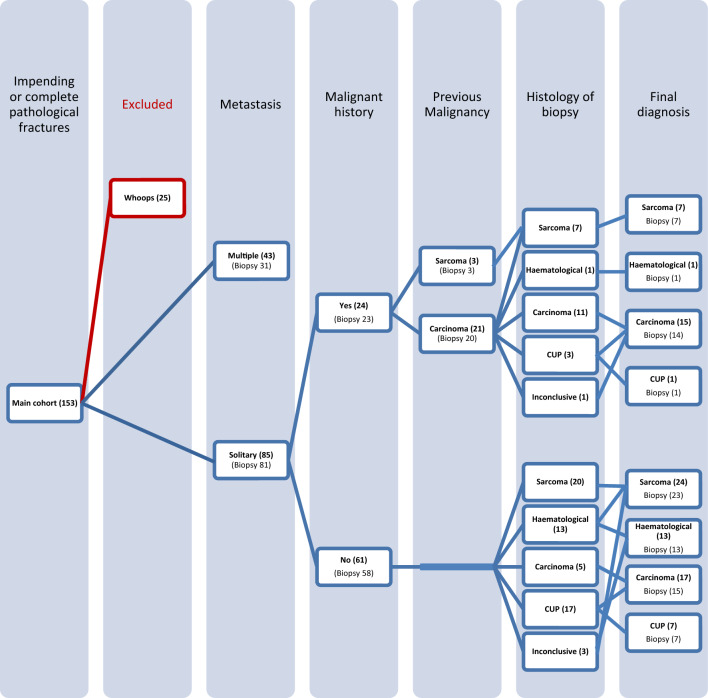
All patients (n = 153) presenting with pathological proximal femoral fractures between 2000 and 2019 were retrospectively evaluated. Patients after inadvertent surgery (n = 25) were excluded. Descriptive statistics were used to evaluate the accuracy and morbidity of diagnostic biopsies.
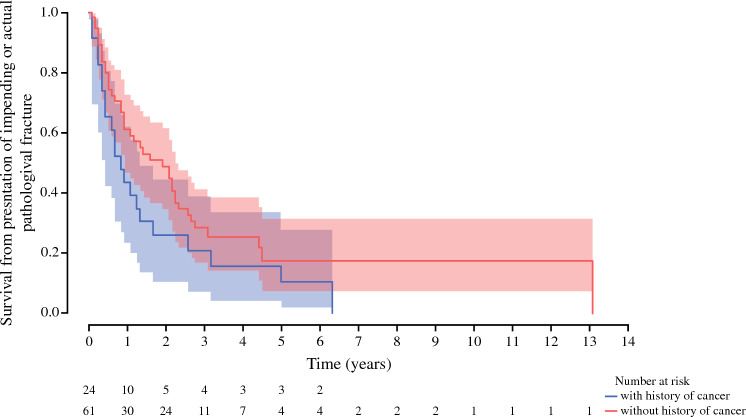
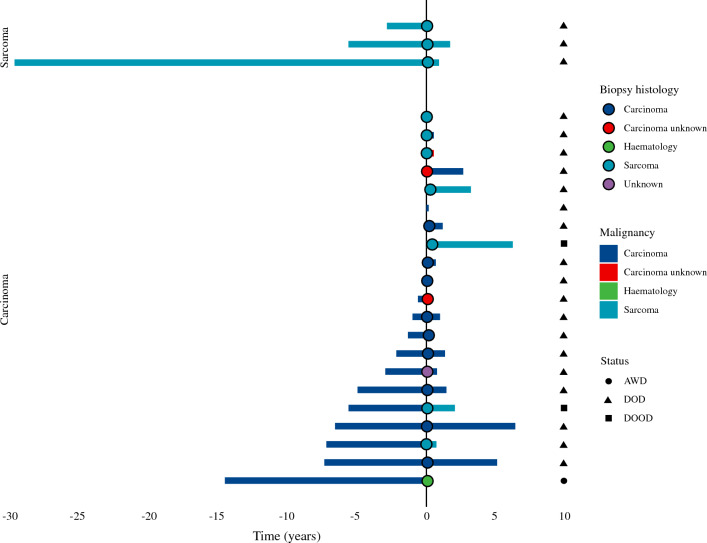
Of 112/128 patients who underwent biopsy, nine (8%) biopsies were unreliable either due to being inconclusive (n = 5) or because the diagnosis changed after resection (n = 4). Of impending fractures, 32% fractured following needle core biopsy. Median time from diagnosis to surgery was 30 days (interquartile range 21-46). The overall biopsy positive predictive value (PPV) to differentiate between sarcoma and non-sarcoma was 1.00 (95% confidence interval [CI] 0.88-1.00). In patients with a previous malignancy (n = 24), biopsy (n = 23) identified the diagnosis in 83% (PPV 0.91, 95% CI 0.71-0.99), of whom five (24%) patients had a new diagnosis. In patients without a history of cancer (n = 61), final diagnosis included carcinomas (n = 24, 39.3%), sarcomas (n = 24, 39.3%), or hematological malignancies (n = 13, 21.3%). Biopsy (n = 58) correctly identified the diagnosis in 66% of patients (PPV 0.80, 95% CI 0.67-0.90).
This study confirms the importance of a preoperative biopsy in solitary pathological proximal femoral fractures due to the risk of sarcoma in patients with and without a history of cancer. However, biopsy delays the time to definite surgery, results can be inconclusive or false, and it risks completion of impending fractures.
对于出现(即将发生和已完全发生的)病理性股骨近端骨折的患者,最佳手术治疗方案取决于预后情况。指南建议进行术前活检以排除肉瘤,但尚无证据证实其益处。
本研究旨在描述这些患者活检结果的诊断准确性、发病率和肉瘤发生率。
对2000年至2019年间出现病理性股骨近端骨折的所有患者(n = 153)进行回顾性评估。排除意外手术后的患者(n = 25)。采用描述性统计方法评估诊断性活检的准确性和发病率。
在128例接受活检的患者中,有112例,其中9例(8%)活检结果不可靠,原因要么是结果不确定(n = 5),要么是切除后诊断发生改变(n = 4)。在即将发生骨折的患者中,32%在针芯活检后发生骨折。从诊断到手术的中位时间为30天(四分位间距21 - 46天)。区分肉瘤和非肉瘤的总体活检阳性预测值(PPV)为1.00(95%置信区间[CI] 0.88 - 1.00)。在有既往恶性肿瘤病史的患者(n = 24)中,活检(n = 23)在83%的患者中明确了诊断(PPV 0.91, 95% CI 0.71 - 0.99),其中5例(24%)患者有新的诊断。在无癌症病史的患者(n = 61)中,最终诊断包括癌(n = 24, 39.)、肉瘤(n = 24, 39.3%)或血液系统恶性肿瘤(n = 13, 21.3%)。活检(n = 58)在66%的患者中正确明确了诊断(PPV 0.80, 95% CI 0.67 - 0.90)。
本研究证实了术前活检在孤立性病理性股骨近端骨折中的重要性,因为无论有无癌症病史的患者都存在肉瘤风险。然而,活检会延迟确定性手术的时间,结果可能不确定或有误,且有导致即将发生的骨折发生的风险。