Department of Pharmacy, Pusan National University Hospital, Pusan, Republic of Korea.
Department of Biostatistics, Clinical Trial Center, Biomedical Research Institute, Pusan National University Hospital, Pusan, Republic of Korea.
Drugs R D. 2023 Sep;23(3):289-296. doi: 10.1007/s40268-023-00436-4. Epub 2023 Jul 28.
Tramadol has been reported to cause hyponatremia but the evidence is conflicting. The risk of hyponatremia resulting from combination oral tramadol/acetaminophen (TA) therapy is thus unknown. This study examined whether, compared with acetaminophen (AA), TA use is associated with an increased risk of hyponatremia.
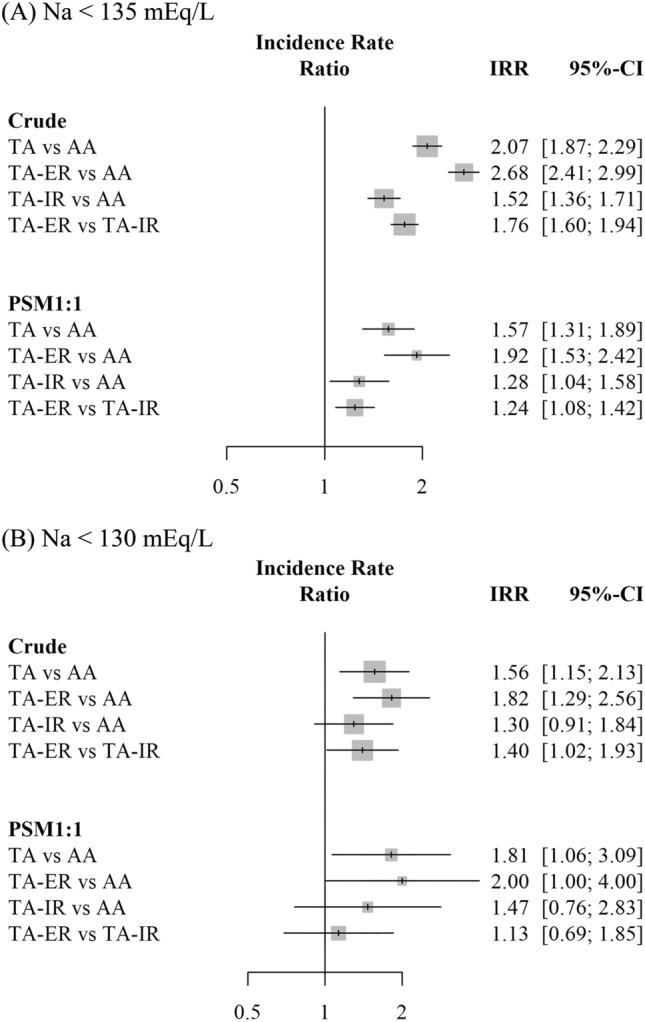
Hospital data compatible with the Observational Medical Outcomes Partnership-Common Data Model (OMOP-CDM; version 5.3) for 30,999 patients taking TA or AA from 2011 through 2020 were analyzed. New-onset hyponatremia was defined as a serum sodium level < 135 mEq/L within 10 days after drug initiation. The incidence rate ratio was calculated based on crude and 1:1 propensity-score-matched models. Subgroup analyses compared patients taking TA extended-release (TA-ER) and TA immediate-release (TA-IR) formulations.
Among the 30,999 patients, 12,122 (39.1%) were aged > 65 years and 16,654 (53.7%) were male. Hyponatremia within 10 days developed in 1613 (8.4%) of the 19,149 patients in the TA group; the incidence rate was higher than in the AA group (4.2%; 493 out of 11,850 cases). In the propensity-score-matched model, the incidence rate of hyponatremia in the TA group was 6.8 per 1000 person-days (PD), which was 1.57-fold (1.31, 1.89) higher than that in the AA group (4.3 per 1000 PD). In both the crude and propensity-score-matched models, the incidence rate of hyponatremia was significantly higher in the TA-ER than TA-IR subgroup.
In this real-world study, hyponatremia was more frequently observed in the TA than AA group, and in the TA-ER than TA-IR subgroup. Therefore, it is imperative to prescribe tramadol cautiously and closely monitor electrolyte levels.
已有报道称曲马多可引起低钠血症,但证据相互矛盾。因此,联合口服曲马多/对乙酰氨基酚(TA)治疗导致低钠血症的风险尚不清楚。本研究旨在评估与对乙酰氨基酚(AA)相比,TA 治疗是否会增加低钠血症的风险。
分析了 2011 年至 2020 年间,符合观察性医疗结局伙伴关系-通用数据模型(OMOP-CDM;版本 5.3)的 30999 例服用 TA 或 AA 的患者数据。新诊断的低钠血症定义为起始药物后 10 天内血清钠水平<135 mEq/L。基于粗模型和 1:1 倾向评分匹配模型计算发病率比值。亚组分析比较了服用 TA 缓释制剂(TA-ER)和 TA 速释制剂(TA-IR)的患者。
在 30999 例患者中,年龄>65 岁的患者有 12122 例(39.1%),男性患者有 16654 例(53.7%)。在 TA 组的 19149 例患者中,10 天内出现低钠血症的患者有 1613 例(8.4%);发生率高于 AA 组(4.2%;493 例/11850 例)。在倾向评分匹配模型中,TA 组低钠血症的发生率为 6.8/1000 人日(PD),是 AA 组(4.3/1000 PD)的 1.57 倍(1.31,1.89)。在粗模型和倾向评分匹配模型中,TA-ER 亚组的低钠血症发生率均显著高于 TA-IR 亚组。
在这项真实世界研究中,与 AA 组相比,TA 组更频繁地观察到低钠血症,与 TA-IR 组相比,TA-ER 组更频繁地观察到低钠血症。因此,谨慎处方曲马多并密切监测电解质水平至关重要。