Ronda Mar, Llop-Talaveron Josep Manuel, Fuset MariPaz, Leiva Elisabet, Shaw Evelyn, Gumucio-Sanguino Victor Daniel, Diez Yolanda, Colom Helena, Rigo-Bonnin Raul, Puig-Asensio Mireia, Carratalà Jordi, Padullés Ariadna
Infectious Disease Department, Hospital Universitari de Bellvitge-IDIBELL, Hospitalet de Llobregat, 08907 Barcelona, Spain.
Pharmacy Department, Hospital Universitari de Bellvitge-IDIBELL, Hospitalet de Llobregat, 08907 Barcelona, Spain.
Antibiotics (Basel). 2023 Jun 25;12(7):1100. doi: 10.3390/antibiotics12071100.
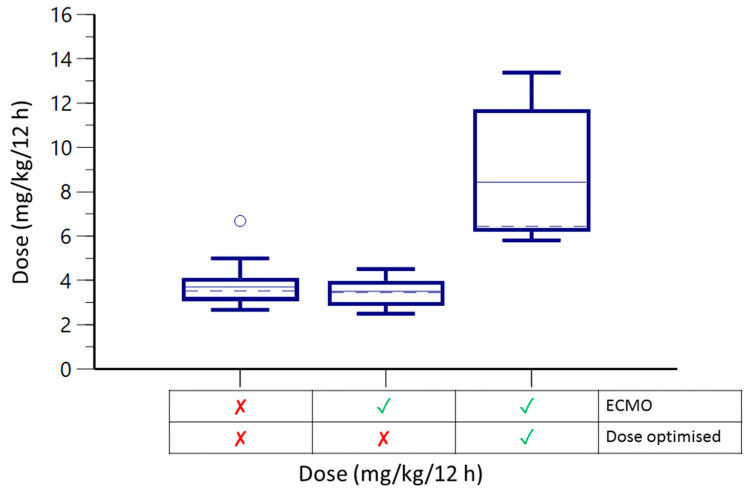
Voriconazole, an antifungal agent, displays high intra- and inter-individual variability. The predictive pharmacokinetic (PK) index requires a minimum plasma concentration (C) in patient serum of between 1-5.5 mg/L. It is common to encounter fungal infections in patients undergoing extracorporeal membrane oxygenation (ECMO) support, and data regarding voriconazole PK changes during ECMO are scarce. Our study compared voriconazole PKs in patients with and without ECMO support in a retrospective cohort of critically-ill patients. Fifteen patients with 26 voriconazole C determinations in the non-ECMO group and nine patients with 27 voriconazole C determinations in the ECMO group were recruited. The ECMO group had lower C (0.38 ± 2.98 vs. 3.62 ± 3.88, < 0.001) and higher infratherapeutic C values (16 vs. 1, < 0.001) than the non-ECMO group. Multivariate analysis identified ECMO support (-0.668, CI -0.978--0.358) and plasma albumin levels (-0.023, CI -0.046--0.001) as risk factors for low C values. When comparing pre- and post-therapeutic drug optimisation samples from the ECMO group, the dose required to achieve therapeutic C was 6.44 mg/kg twice a day. Therapeutic drug optimisation is essential to improve target attainment.
伏立康唑是一种抗真菌药物,在个体内和个体间显示出高度变异性。预测性药代动力学(PK)指标要求患者血清中的最低血浆浓度(C)在1 - 5.5毫克/升之间。接受体外膜肺氧合(ECMO)支持的患者中常见真菌感染,而关于ECMO期间伏立康唑PK变化的数据很少。我们的研究在一组重症患者的回顾性队列中比较了有和没有ECMO支持的患者的伏立康唑PK。非ECMO组招募了15名患者,进行了26次伏立康唑C测定,ECMO组招募了9名患者,进行了27次伏立康唑C测定。与非ECMO组相比,ECMO组的C较低(0.38±2.98 vs. 3.62±3.88,<0.001),治疗不足的C值较高(16 vs. 1,<0.001)。多变量分析确定ECMO支持(-0.668,CI -0.978--0.358)和血浆白蛋白水平(-0.023,CI -0.046--0.001)是低C值的危险因素。比较ECMO组治疗前和治疗后药物优化样本时,达到治疗性C所需的剂量为每天两次6.44毫克/千克。治疗药物优化对于提高目标达成至关重要。