Sakurai Yuto, Ebihara Yuma, Kurashima Yo, Murakami Soichi, Shichinohe Toshiaki, Hirano Satoshi
Department of Gastroenterological Surgery II, Hokkaido University Faculty of Medicine, North 15 West 7, Kita-ku, Sapporo 0608638, Hokkaido, Japan.
Department of Gastroenterological Surgery II, Hokkaido University Faculty of Medicine, North 15 West 7, Kita-ku, Sapporo 0608638, Hokkaido, Japan.
Int J Surg Case Rep. 2023 Aug;109:108561. doi: 10.1016/j.ijscr.2023.108561. Epub 2023 Jul 21.
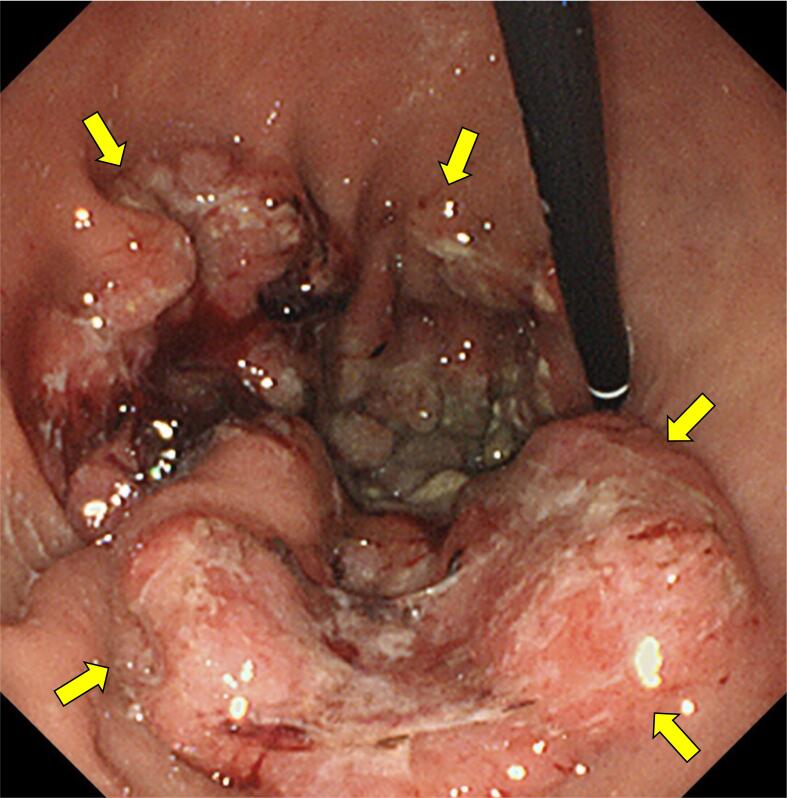
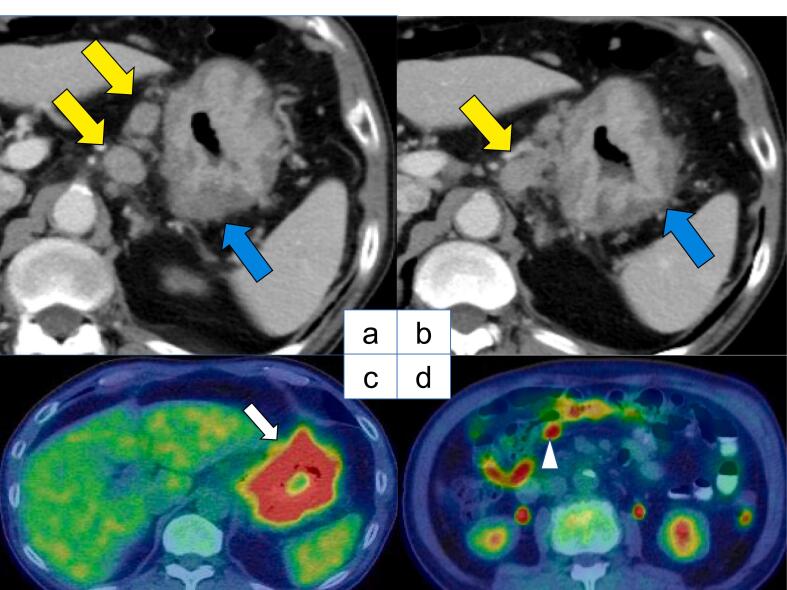
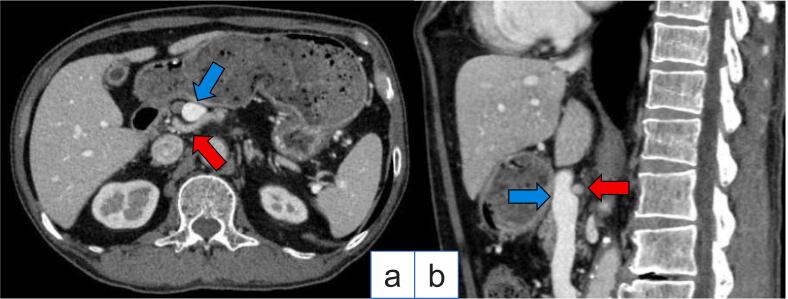
It is essential to identify variations of celiac artery (CA) and common hepatic artery (CHA), using preoperative computed tomography (CT) imaging, for safe gastrectomy and lymph node dissection in gastric cancer (GC) surgery. We report a relatively rare case with the CHA passing behind the portal vein (PV), in which we performed robot-assisted total gastrectomy (RTG) after chemotherapy as conversion surgery.
A 78-year-old man with GC was referred for conversion surgery. Three-dimensional CT angiography revealed an anomalous CHA passing behind the PV. The anomaly corresponded to type I according to Adachi's classification, and the patient underwent robot-assisted laparoscopic total gastrectomy D2 lymphadenectomy (RTG D2) with Roux-en-Y reconstruction. The operation time was 543 min, blood loss was 115 ml, and no intraoperative complications occurred. The postoperative course was uneventful.
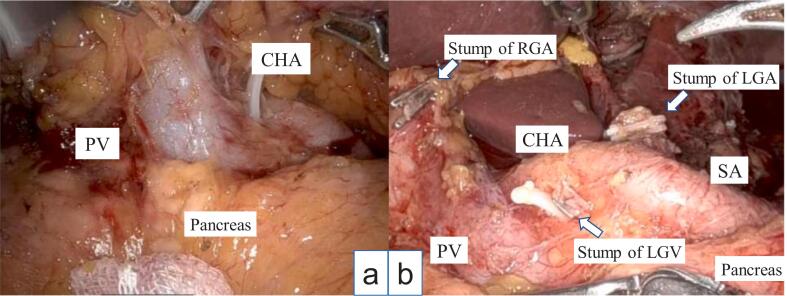
A word of caution during the surgical procedure entails the manipulation of the suprapancreatic lymph node dissection. Initially, it is crucial to identify the anterior surface of the portal vein (PV) and the nerve plexus surrounding the common hepatic artery (CHA). After completely dissecting the entire circumference, the PV is secured using vascular tape. By gently pulling the vascular tape towards the ventral aspect, a safe execution of lymph node dissection no.8 and 12 on the dorsal side of the PV can be accomplished. Meticulous handling of the anatomical abnormalities observed in the preoperative images may prevent unintended hemorrhage.
We report a case with vascular anomalies in which RTG D2 was performed successfully as a conversion surgery.
在胃癌(GC)手术中,为了安全地进行胃切除术和淋巴结清扫,利用术前计算机断层扫描(CT)成像识别腹腔干(CA)和肝总动脉(CHA)的变异至关重要。我们报告了1例相对罕见的肝总动脉从门静脉(PV)后方经过的病例,该患者在化疗后作为挽救性手术接受了机器人辅助全胃切除术(RTG)。
一名78岁的GC男性患者被转诊进行挽救性手术。三维CT血管造影显示肝总动脉异常从门静脉后方经过。根据安达氏分类,该异常属于I型,患者接受了机器人辅助腹腔镜全胃切除术D2淋巴结清扫术(RTG D2)并进行了Roux-en-Y重建。手术时间为543分钟,出血量为115毫升,术中未发生并发症。术后恢复顺利。
手术过程中的一个注意事项是胰上淋巴结清扫的操作。首先,识别门静脉(PV)的前表面和肝总动脉(CHA)周围的神经丛至关重要。在完全解剖整个圆周后,用血管带固定门静脉。通过轻轻将血管带拉向腹侧,可以安全地在门静脉背侧进行第8组和第12组淋巴结清扫。仔细处理术前图像中观察到的解剖异常可能会防止意外出血。
我们报告了1例血管异常病例,其中成功地将RTG D2作为挽救性手术进行。