Department of Translational Medicine, Division of Medical Radiology, University of Lund, Malmö, Sweden.
Department of Surgical Sciences, Section of Radiology, Uppsala University, Uppsala, Sweden.
Eur Radiol. 2024 Jan;34(1):612-621. doi: 10.1007/s00330-023-09962-w. Epub 2023 Aug 4.
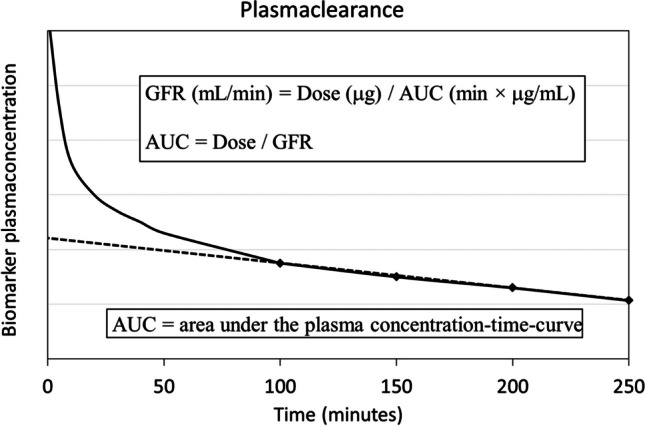
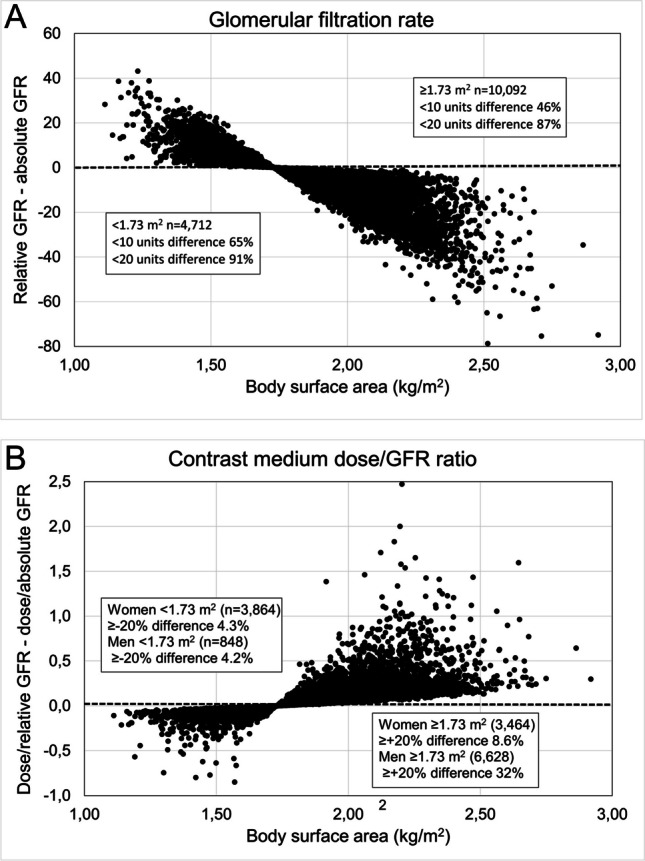
Glomerular filtration rate (GFR) is considered the best overall index of kidney function in health and disease and its use is recommended to evaluate the risk of iodine contrast medium-induced acute kidney injury (CI-AKI) either as a single parameter or as a ratio between the total contrast medium dose (gram iodine) and GFR. GFR may be expressed in absolute terms (mL/min) or adjusted/indexed to body surface area, relative GFR (mL/min/1.73 m). Absolute and relative GFR have been used interchangeably to evaluate the risk of CI-AKI, which may be confusing and a potential source of errors. Relative GFR should be used to assess the GFR category of renal function as a sign of the degree of kidney damage and sensitivity for CI-AKI. Absolute GFR represents the excretion capacity of the individual and may be used to calculate the gram-iodine/absolute GFR ratio, an index of systemic drug exposure (amount of contrast medium in the body) that relates to toxicity. It has been found to be an independent predictor of AKI following percutaneous coronary angiography and interventions but has not yet been fully validated for computed tomography (CT). Prospective studies are warranted to evaluate the optimal gram-iodine/absolute GFR ratio to predict AKI at various stages of renal function at CT. Only GFR estimation (eGFR) equations based on standardized creatinine and/or cystatin C assays should be used. eGFR/eGFR ratio < 0.6 indicating selective glomerular hypofiltration syndrome may have a stronger predictive power for postcontrast AKI than creatinine-based eGFR. CLINICAL RELEVANCE STATEMENT: Once the degree of kidney damage is established by estimating relative GFR (mL/min/1.73 m), contrast dose in relation to renal excretion capacity [gram-iodine/absolute GFR (mL/min)] may be the best index to evaluate the risk of contrast-induced kidney injury. KEY POINTS: • Relative glomerular filtration rate (GFR; mL/min/1.73 m) should be used to assess the GFR category as a sign of the degree of kidney damage and sensitivity to contrast medium-induced acute kidney injury (CI-AKI). • Absolute GFR (mL/min) is the individual's actual excretion capacity and the contrast-dose/absolute GFR ratio is a measure of systemic exposure (amount of contrast medium in the body), relates to toxicity and should be expressed in gram-iodine/absolute GFR (mL/min). • Prospective studies are warranted to evaluate the optimal contrast medium dose/GFR ratio predicting the risk of CI-AKI at CT and intra-arterial examinations.
肾小球滤过率(GFR)被认为是健康和疾病中评估肾脏功能的最佳综合指标,建议使用它来评估碘对比剂引起的急性肾损伤(CI-AKI)的风险,无论是作为单一参数还是作为总对比剂剂量(克碘)与 GFR 的比值。GFR 可以用绝对值(mL/min)表示,也可以用体表面积校正/指数化,相对 GFR(mL/min/1.73 m)。绝对 GFR 和相对 GFR 可互换用于评估 CI-AKI 的风险,这可能会令人困惑,并且是潜在的错误来源。相对 GFR 应用于评估肾功能的 GFR 类别,作为肾脏损伤程度和对 CI-AKI 敏感性的标志。绝对 GFR 代表个体的排泄能力,可用于计算克碘/绝对 GFR 比值,这是全身药物暴露(体内的对比剂量)的指标,与毒性有关。已经发现它是经皮冠状动脉血管造影和介入后 AKI 的独立预测因子,但尚未在 CT 方面得到充分验证。需要进行前瞻性研究来评估在 CT 时各种肾功能阶段预测 AKI 的最佳克碘/绝对 GFR 比值。仅应使用基于标准化肌酐和/或胱抑素 C 检测的 GFR 估计(eGFR)方程。指示选择性肾小球滤过率降低综合征的 eGFR/eGFR 比值 < 0.6 可能对造影后 AKI 具有比基于肌酐的 eGFR 更强的预测能力。临床意义:一旦通过估计相对 GFR(mL/min/1.73 m)确定了肾脏损伤程度,就可以根据肾排泄能力[克碘/绝对 GFR(mL/min)]来评估对比剂引起的肾损伤的风险。关键要点:•相对肾小球滤过率(GFR;mL/min/1.73 m)应用于评估 GFR 类别,作为肾脏损伤程度和对造影剂引起的急性肾损伤(CI-AKI)敏感性的标志。•绝对 GFR(mL/min)是个体的实际排泄能力,而对比剂剂量/绝对 GFR 比值是全身暴露(体内的对比剂量)的量度,与毒性有关,应表示为克碘/绝对 GFR(mL/min)。•需要进行前瞻性研究来评估预测 CT 和动脉内检查中 CI-AKI 风险的最佳对比剂剂量/GFR 比值。