Regional Epilepsy Center, Neurology Unit, San Bortolo Hospital, Vicenza, Italy.
Science of Health Department, School of Medicine, Magna Graecia University of Catanzaro, Via T. Campanella, 115, 88100, Catanzaro, Italy.
Neurol Sci. 2024 Jan;45(1):277-288. doi: 10.1007/s10072-023-06992-6. Epub 2023 Aug 7.
There is little and controversial information about changes in plasma concentrations (PCs) or clinical events during coadministration of antiseizure medications (ASMs) and direct oral anticoagulants (DOACs). We aimed to explore possible determinants of dosage class among DOACs trough PCs when ASMs are co-administered and the relative risks. We also provided some clinical examples of patients' management.
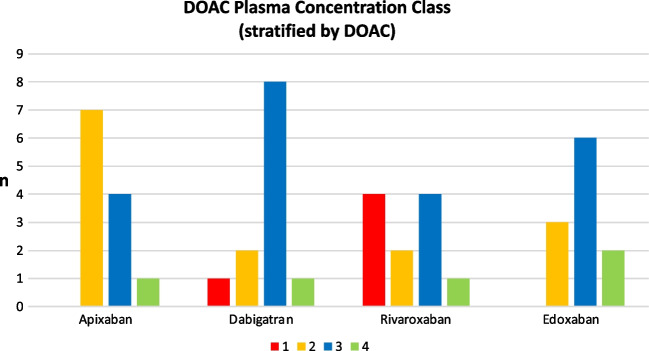
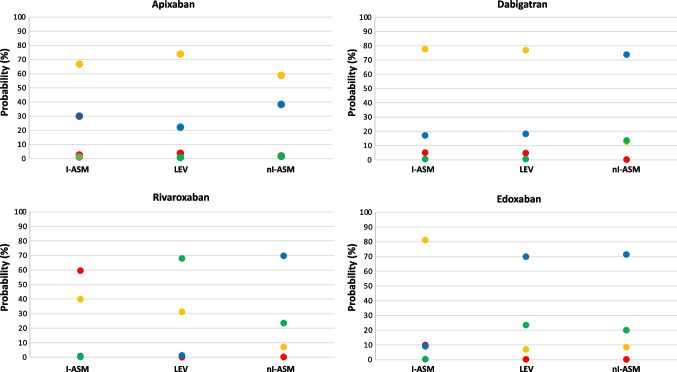
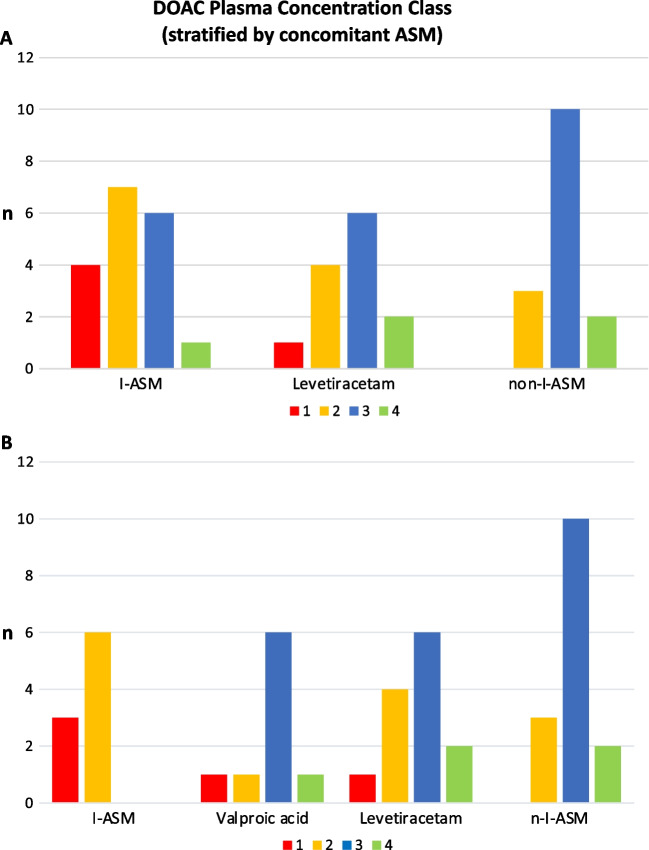
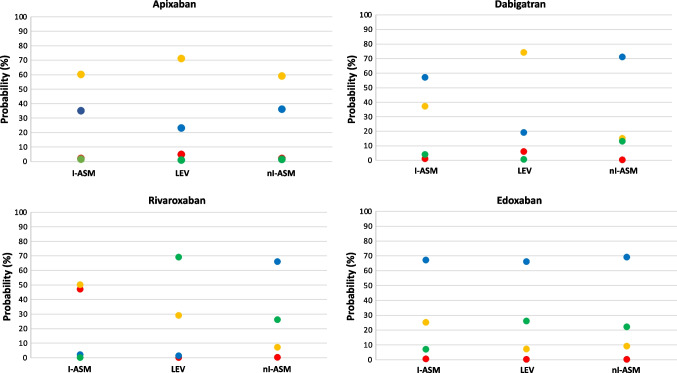
Data on adult patients concomitantly treated with ASMs (grouped in enzyme-inducing [I-ASMs], non-inducing [nI-ASMs], and levetiracetam [LEV]) and DOACs with at least one measurement of DOACs' PC were retrospectively collected. The role of DOAC-ASM combinations in predicting PC class (ranging from I at ischemic/thromboembolic risk to IV at increased bleeding risk) was investigated by an ordered logit model, and the marginal probabilities of belonging to the four dosage classes were calculated.
We collected 46 DOACs' PCs out of 31 patients. There were 5 (10.9%) determinations in class I (4 out of 5 with concomitant I-ASMs) and 5 (10.9%) in class IV. The rivaroxaban/I-ASM combination was associated with lower DOAC dosages than rivaroxaban/LEV (OR: 0.00; 95% CI: 0.00-0.62). Furthermore, patient's probability of being in class I was approximately 50% with the rivaroxaban/I-ASM combination, while apixaban, dabigatran, and edoxaban had the highest cumulative probability of being in class II or III despite the ASM used.
These preliminary results confirm the reduction of DOAC's PC by I-ASMs and suggest a better manageability of apixaban, dabigatran, and edoxaban independently from the concomitant ASM, whereas rivaroxaban seems the most liable to PC alterations with I-ASMs.
抗癫痫药物(ASMs)与直接口服抗凝剂(DOACs)合用时,关于血浆浓度(PCs)变化或临床事件的信息很少且存在争议。我们旨在探讨 ASMs 合用时 DOACs 谷浓度(PCs)的剂量类别可能的决定因素及其相对风险。我们还提供了一些患者管理的临床实例。
回顾性收集同时接受 ASMs(分为酶诱导 [I-ASM]、非诱导 [nI-ASM] 和左乙拉西坦 [LEV])和至少一次 DOACs PC 测量的成年患者的数据。通过有序逻辑回归模型研究 DOAC-ASM 组合在预测 PC 类别(从缺血/血栓栓塞风险的 I 类到增加出血风险的 IV 类)中的作用,并计算属于四个剂量类别的边际概率。
我们从 31 名患者中收集了 46 个 DOACs 的 PC。其中 5 个(5 个中有 4 个与 I-ASM 同时存在)处于 I 类,5 个(5 个中有 4 个与 LEV 同时存在)处于 IV 类。利伐沙班/I-ASM 联合与利伐沙班/LEV 相比,DOAC 剂量较低(OR:0.00;95%CI:0.00-0.62)。此外,利伐沙班/I-ASM 联合治疗时,患者处于 I 类的概率约为 50%,而阿哌沙班、达比加群和依度沙班尽管使用了 ASM,但处于 II 类或 III 类的累积概率最高。
这些初步结果证实 I-ASM 可降低 DOAC 的 PC,并表明阿哌沙班、达比加群和依度沙班在不依赖同时使用的 ASM 的情况下更易于管理,而利伐沙班似乎最容易因 I-ASM 而改变 PC。