Scheese Daniel, Alwatari Yahya, Rustom Salem, He Gene, Puig Carlos A, Julliard Walker A, Shah Rachit D
Virginia Commonwealth University, Section of Thoracic & Foregut Surgery, Department of Surgery, Richmond, VA, USA.
J Thorac Dis. 2023 Jul 31;15(7):3593-3604. doi: 10.21037/jtd-23-37. Epub 2023 Jul 3.
Anastomotic leak is a major contributor to comorbidity and mortality following esophagectomy. We sought to assess rate and predictors of leak after esophagectomy and compare outcomes of chest versus neck anastomotic leaks.
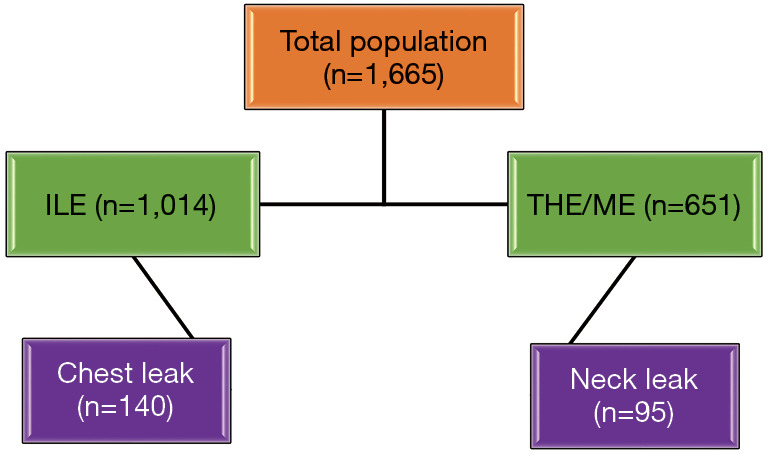
A retrospective review was performed utilizing National-Surgical-Quality-Improvement-Program data from 2016-2019 for patients undergoing esophagectomy for malignancy. Preoperative characteristics and postoperative outcomes were compared. Patients were classified into two groups: Ivor Lewis esophagectomy [ILE, chest leak (CL)] and transhiatal esophagectomy (THE)/McKeown esophagectomy [ME, neck leak (NL)]. Multivariable regression models were constructed to determine predictors of each type of leak and postoperative complications.
A total of 1,665 patients underwent esophagectomy with 14.1% reported post-operative leak, 61% of patients underwent ILE while 39% underwent THE or ME. Of patients who underwent ILE, 13.8% had CL with complications including significantly higher length of stay and mortality compared to patients without leak. Independent predictors of CL included: diabetes, hypertension, advanced disease stage, chronic steroid use, and operative time. Ninety-five patients (14.6%) who underwent either THE or ME had NL with similar complications. Diabetes, pre-operative white blood cell (WBC), and operative time were independent predictors for NL. On multivariable regression, CL was associated with greater odds of requiring intervention compared with NL.
Post-esophagectomy CL and NL are associated with higher morbidity and mortality. Diabetes and operative time were independent predictors for both leaks while steroid use, hypertension, and advanced disease stage predicted CL. CL was associated with greater odds of needing an intervention, but contrary to conventional wisdom, was not associated with higher morbidity or mortality.
吻合口漏是食管切除术后合并症和死亡率的主要原因。我们试图评估食管切除术后漏的发生率和预测因素,并比较胸段与颈段吻合口漏的结果。
利用2016 - 2019年国家外科质量改进计划数据,对因恶性肿瘤接受食管切除术的患者进行回顾性研究。比较术前特征和术后结果。患者分为两组:艾弗·刘易斯食管切除术[ILE,胸段漏(CL)]和经裂孔食管切除术(THE)/麦克基翁食管切除术[ME,颈段漏(NL)]。构建多变量回归模型以确定每种类型漏和术后并发症的预测因素。
共有1665例患者接受了食管切除术,14.1%报告有术后漏,61%的患者接受ILE,39%的患者接受THE或ME。接受ILE的患者中,13.8%发生CL,其并发症包括与无漏患者相比住院时间显著延长和死亡率更高。CL的独立预测因素包括:糖尿病、高血压、疾病晚期、长期使用类固醇和手术时间。95例(14.6%)接受THE或ME的患者发生NL,并发症相似。糖尿病、术前白细胞(WBC)和手术时间是NL的独立预测因素。在多变量回归分析中,与NL相比,CL需要干预的几率更高。
食管切除术后CL和NL与更高的发病率和死亡率相关。糖尿病和手术时间是两种漏的独立预测因素,而类固醇使用、高血压和疾病晚期预测CL。CL需要干预的几率更高,但与传统观念相反,与更高的发病率或死亡率无关。