Department of Anesthesiology, Washington University School of Medicine, St Louis, Missouri.
Institute for Informatics, Washington University School of Medicine, St Louis, Missouri.
JAMA Netw Open. 2023 Aug 1;6(8):e2328514. doi: 10.1001/jamanetworkopen.2023.28514.
Accurate measurements of clinical workload are needed to inform health care policy. Existing methods for measuring clinical workload rely on surveys or time-motion studies, which are labor-intensive to collect and subject to biases.
To compare anesthesia clinical workload estimated from electronic health record (EHR) audit log data vs billed relative value units.
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study of anesthetic encounters occurring between August 26, 2019, and February 9, 2020, used data from 8 academic hospitals, community hospitals, and surgical centers across Missouri and Illinois. Clinicians who provided anesthetic services for at least 1 surgical encounter were included. Data were analyzed from January 2022 to January 2023.
Anesthetic encounters associated with a surgical procedure were included. Encounters associated with labor analgesia and endoscopy were excluded.
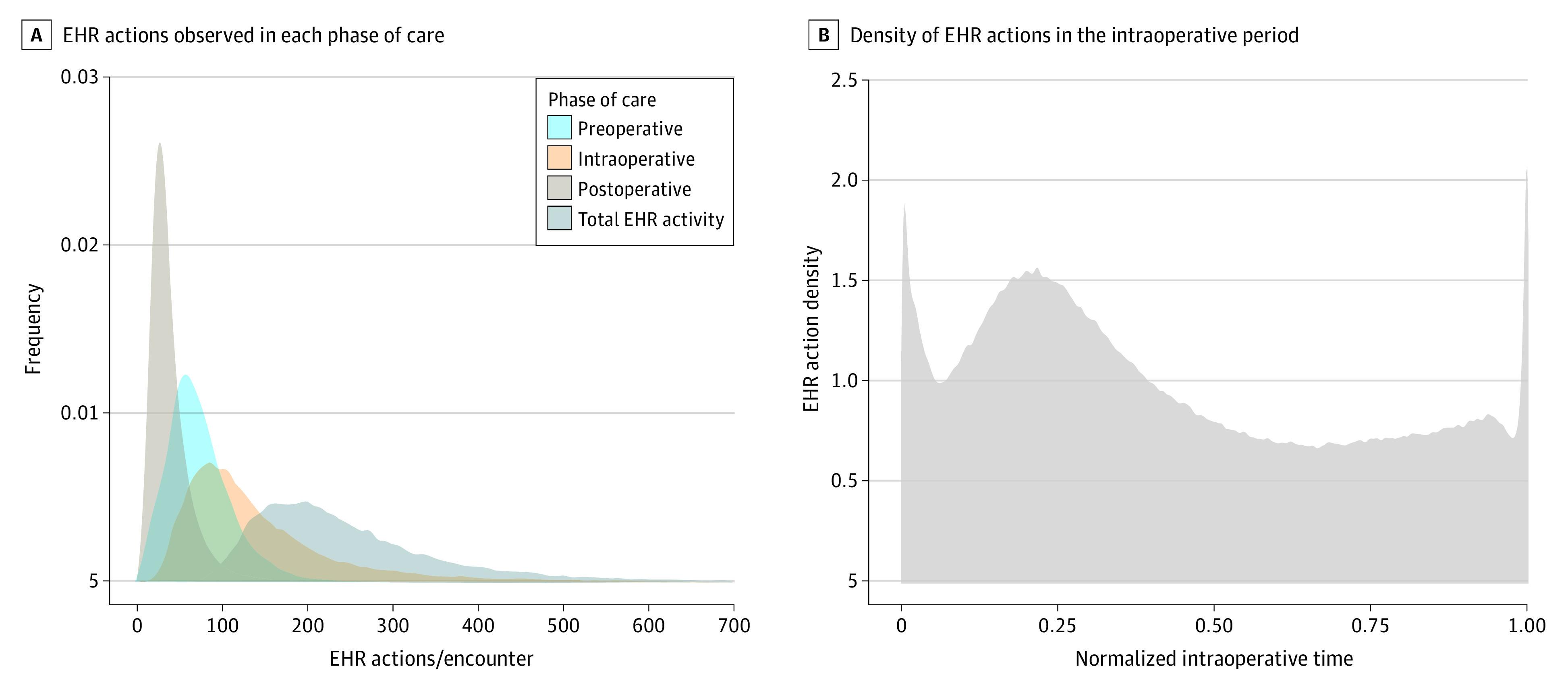
For each encounter, EHR-derived clinical workload was estimated as the sum of all EHR actions recorded in the audit log by anesthesia clinicians who provided care. Billing-derived clinical workload was measured as the total number of units billed for the encounter. A linear mixed-effects model was used to estimate the relative contribution of patient complexity (American Society of Anesthesiology [ASA] physical status modifier), procedure complexity (ASA base unit value for the procedure), and anesthetic duration (time units) to EHR-derived and billing-derived workload. The resulting β coefficients were interpreted as the expected effect of a 1-unit change in each independent variable on the standardized workload outcome. The analysis plan was developed after the data were obtained.
A total of 405 clinicians who provided anesthesia for 31 688 encounters were included in the study. A total of 8 288 132 audit log actions corresponding to 39 131 hours of EHR use were used to measure EHR-derived workload. The contributions of patient complexity, procedural complexity, and anesthesia duration to EHR-derived workload differed significantly from their contributions to billing-derived workload. The contribution of patient complexity toward EHR-derived workload (β = 0.162; 95% CI, 0.153-0.171) was more than 50% greater than its contribution toward billing-derived workload (β = 0.106; 95% CI, 0.097-0.116; P < .001). In contrast, the contribution of procedure complexity toward EHR-derived workload (β = 0.033; 95% CI, 0.031-0.035) was approximately one-third its contribution toward billing-derived workload (β = 0.106; 95% CI, 0.104-0.108; P < .001).
In this cross-sectional study of 8 hospitals, reimbursement for anesthesiology services overcompensated for procedural complexity and undercompensated for patient complexity. This method for measuring clinical workload could be used to improve reimbursement valuations for anesthesia and other specialties.
需要准确测量临床工作量,以为医疗保健政策提供信息。现有的临床工作量测量方法依赖于调查或时间运动研究,这些方法收集起来既费力又容易受到偏差的影响。
比较从电子健康记录(EHR)审计日志数据和计费相对价值单位(RVU)估算的麻醉临床工作量。
设计、设置和参与者:这是一项在 2019 年 8 月 26 日至 2020 年 2 月 9 日期间发生的麻醉手术的横断面研究,使用了来自密苏里州和伊利诺伊州的 8 家学术医院、社区医院和外科中心的数据。研究对象为至少进行了 1 次手术的麻醉医师。数据分析于 2022 年 1 月至 2023 年 1 月进行。
纳入与手术相关的麻醉手术。排除与分娩镇痛和内窥镜检查相关的手术。
对于每个手术,通过 EHR 记录的所有 EHR 操作的总和来估计 EHR 衍生的临床工作量,这些操作由提供护理的麻醉临床医生记录。计费衍生的临床工作量通过计费的总单位数来衡量。使用线性混合效应模型来估计患者复杂性(美国麻醉医师协会 [ASA] 身体状况修正)、手术复杂性(ASA 基础手术单位值)和麻醉持续时间(时间单位)对 EHR 衍生和计费衍生工作量的相对贡献。由此产生的β系数被解释为每个独立变量增加 1 个单位对标准化工作量结果的预期影响。该分析计划是在获得数据后制定的。
共有 405 名麻醉师为 31688 次手术提供了服务,被纳入了研究。共使用了 8288132 次审计日志操作,对应 39131 小时的 EHR 使用,用于测量 EHR 衍生的工作量。患者复杂性、手术复杂性和麻醉持续时间对 EHR 衍生工作量的贡献与对计费衍生工作量的贡献有显著差异。患者复杂性对 EHR 衍生工作量的贡献(β=0.162;95%置信区间,0.153-0.171)比其对计费衍生工作量的贡献(β=0.106;95%置信区间,0.097-0.116;P<0.001)高出 50%以上。相比之下,手术复杂性对 EHR 衍生工作量的贡献(β=0.033;95%置信区间,0.031-0.035)约为其对计费衍生工作量的贡献的三分之一(β=0.106;95%置信区间,0.104-0.108;P<0.001)。
在这项对 8 家医院的横断面研究中,麻醉服务的报销补偿过度补偿了手术复杂性,而低估了患者复杂性。这种测量临床工作量的方法可用于改进对麻醉和其他专业的报销评估。


