Yaacobi Eyal, Shachar Tal, Segal David, Agabaria Altaieb, Halima Golan, Marom Omer, Ohana Nissim
Department of Orthopaedic Surgery, Meir Medical Center, Tschernihovski 59 Street, Kfar-Saba 4428164, Israel.
Faculty of Medicine, Ramat Aviv, Tel Aviv 69978, Israel.
J Clin Med. 2023 Jul 25;12(15):4880. doi: 10.3390/jcm12154880.
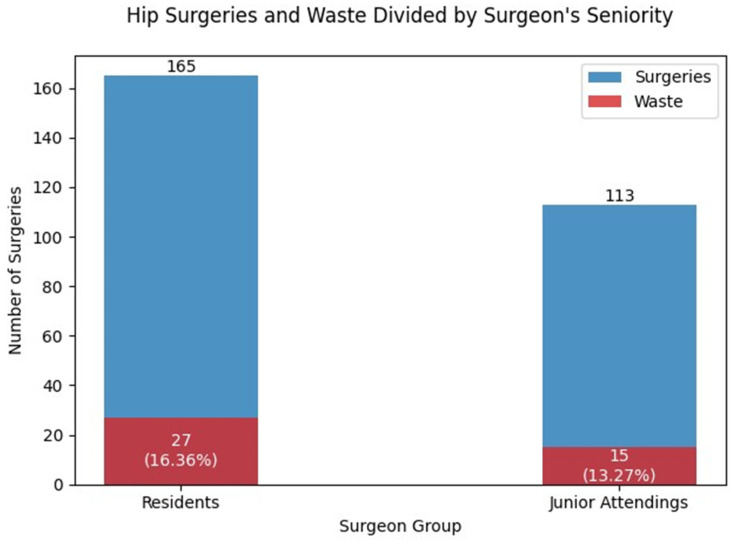
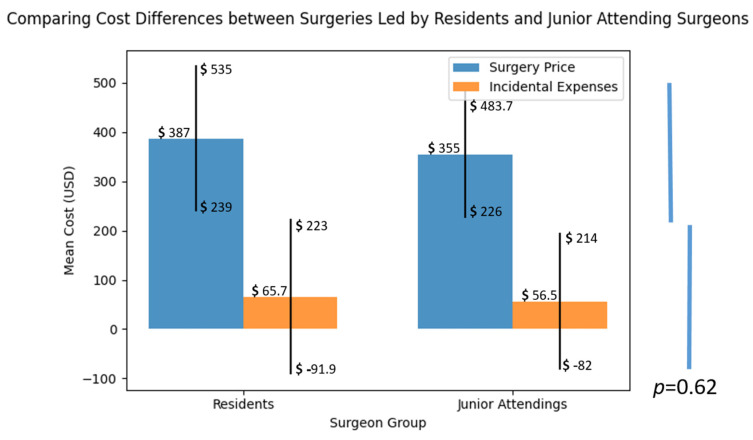
Can the financial impact of implant choice during the learning curve of inexperienced surgeons in hip fracture surgery be quantified? Hip fractures in the elderly are a significant medical concern, often requiring surgical interventions performed by orthopedic surgery residents. As healthcare costs rise, exploring cost reduction opportunities within the healthcare system becomes crucial. In this prospective analysis, we examined the financial implications of implant choices encountered by residents during their learning curve in hip fracture surgery. Our study included 278 surgically treated pertrochanteric fractures using the same locking cephalomedullary nail. Data on patients, surgeons (including their experience and seniority), and all implants charged by the hospital were collected. This encompassed documentation of any nail-related equipment that was opened on the operating table and whether it was subsequently used by the end of the procedure. By calculating the number and cost of these implants, we assessed the financial burden associated with suboptimal choices made during the learning curve. Our findings revealed that in 16.18% of surgeries, instances of suboptimal implant utilization occurred, highlighting the complexities of the learning process. Importantly, the rate of these challenges was not influenced by surgeon seniority or patient characteristics. The mean additional cost per surgery was determined to be USD 65.69 ± 157.63 for surgeries with suboptimal implant utilization, compared to USD 56.55 ± 139.13 for surgeries without such challenges. Although there was a trend towards higher implant-related costs in resident-led surgeries, the difference did not reach statistical significance. These findings underscore the feasibility of enabling residents to autonomously perform intramedullary nailing surgeries, even without specialist supervision, while incurring minimal additional expenses during the learning curve. By acknowledging the financial implications associated with the learning curve in the management of hip fractures, we can strive to optimize healthcare costs, thus addressing an important aspect of this issue.
在经验不足的外科医生进行髋部骨折手术的学习曲线期间,植入物选择所产生的财务影响能否被量化?老年人髋部骨折是一个重大的医学问题,通常需要骨科住院医师进行手术干预。随着医疗成本的上升,探索医疗系统内的成本降低机会变得至关重要。在这项前瞻性分析中,我们研究了住院医师在髋部骨折手术学习曲线期间遇到的植入物选择所带来的财务影响。我们的研究纳入了278例使用同一锁定髓内钉进行手术治疗的转子间骨折。收集了患者、外科医生(包括他们的经验和资历)以及医院收取费用的所有植入物的数据。这包括记录在手术台上打开的任何与钉子相关的设备,以及在手术结束时是否随后被使用。通过计算这些植入物的数量和成本,我们评估了在学习曲线期间因选择不当而产生的财务负担。我们的研究结果显示,在16.18%的手术中,出现了植入物使用不当的情况,凸显了学习过程的复杂性。重要的是,这些挑战的发生率不受外科医生资历或患者特征的影响。与没有此类挑战的手术相比,植入物使用不当的手术每次手术的平均额外成本为65.69美元±157.63美元,而没有此类挑战的手术为56.55美元±139.13美元。尽管在住院医师主导的手术中,与植入物相关的成本有上升趋势,但差异未达到统计学显著性。这些研究结果强调了即使在没有专家监督的情况下,让住院医师自主进行髓内钉手术的可行性,同时在学习曲线期间产生的额外费用最小。通过认识到髋部骨折管理中学习曲线所带来的财务影响,我们可以努力优化医疗成本,从而解决这个问题的一个重要方面。