Morrison Laura, Okines Alicia
Breast Unit, The Royal Marsden NHS Foundation Trust, London SW3 6JJ, UK.
Cancers (Basel). 2023 Jul 26;15(15):3801. doi: 10.3390/cancers15153801.
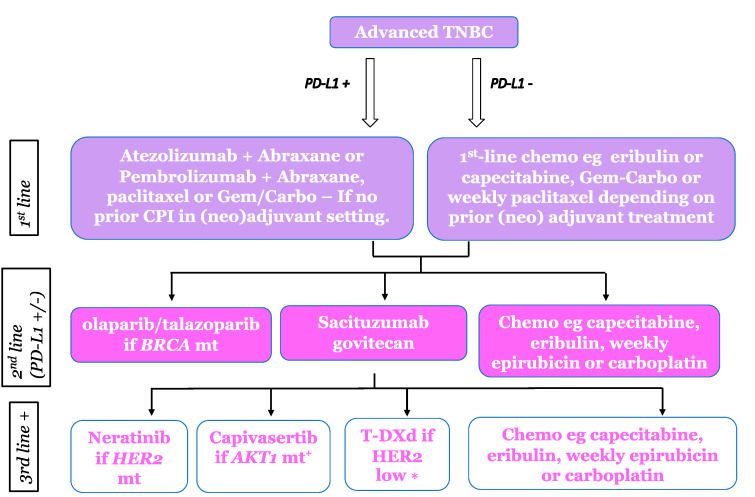
Until recently, despite its heterogenous biology, metastatic triple negative breast cancer (TNBC) was treated as a single entity, with successive lines of palliative chemotherapy being the only systemic option. Significant gene expression studies have demonstrated the diversity of TNBC, but effective differential targeting of the four main (Basal-like 1 and 2, mesenchymal and luminal androgen receptor) molecular sub-types has largely eluded researchers. The introduction of immunotherapy, currently useful only for patients with PD-L1 positive cancers, led to the stratification of first-line therapy using this immunohistochemical biomarker. Germline gene mutations can also be targeted with PARP inhibitors in both the adjuvant and metastatic settings. In contrast, the benefit of the anti-Trop-2 antibody-drug conjugate (ADC) Sacituzumab govitecan (SG) does not appear confined to patients with tumours expressing high levels of Trop-2, leading to its potential utility for any patient with an estrogen receptor (ER)-negative, HER2-negative advanced breast cancer (ABC). Most recently, low levels of HER2 expression, detected in up to 60% of TNBC, predicts benefit from the potent HER2-directed antibody-drug conjugate trastuzumab deruxtecan (T-DXd), defining an additional treatment option for this sub-group. Regrettably, despite recent advances, the median survival of TNBC continues to lag far behind the approximately 5 years now expected for patients with ER-positive or HER2-positive breast cancers. We review the data supporting immunotherapy, ADCs, and targeted agents in subgroups of patients with TNBC, and current clinical trials that may pave the way to further advances in this challenging disease.
直到最近,尽管转移性三阴性乳腺癌(TNBC)生物学特性异质性强,但仍被视为一个单一实体,连续多线姑息化疗是唯一的全身治疗选择。大量基因表达研究已证明TNBC的多样性,但对四种主要分子亚型(基底样1型和2型、间充质型和腔面雄激素受体型)进行有效的差异靶向治疗在很大程度上仍未实现。免疫疗法的引入,目前仅对PD-L1阳性癌症患者有用,导致使用这种免疫组化生物标志物对一线治疗进行分层。在辅助治疗和转移治疗中,胚系基因突变也可用PARP抑制剂进行靶向治疗。相比之下,抗Trop-2抗体药物偶联物(ADC)戈沙妥珠单抗(SG)的益处似乎并不局限于Trop-2表达水平高的肿瘤患者,这使其对任何雌激素受体(ER)阴性、人表皮生长因子受体2(HER2)阴性的晚期乳腺癌(ABC)患者都具有潜在效用。最近,在高达60%的TNBC中检测到的低水平HER2表达预示着可从强效的HER2导向抗体药物偶联物德曲妥珠单抗(T-DXd)中获益,这为该亚组患者定义了另一种治疗选择。遗憾的是,尽管最近取得了进展,但TNBC的中位生存期仍远远落后于ER阳性或HER2阳性乳腺癌患者目前预期的约5年生存期。我们回顾了支持TNBC患者亚组免疫疗法、ADC和靶向药物的数据,以及可能为这种具有挑战性的疾病取得进一步进展铺平道路的当前临床试验。