Research Unit for General Practice, Bartholins Allé 2, 8000, Aarhus C, Denmark.
Department of Public Health, Aarhus University, Aarhus C, Denmark.
BMC Med. 2023 Aug 15;21(1):305. doi: 10.1186/s12916-023-03021-3.
Patients with multimorbidity are frequent users of healthcare, but fragmented care may lead to suboptimal treatment. Yet, this has never been examined across healthcare sectors on a national scale. We aimed to quantify care fragmentation using various measures and to analyze the associations with patient outcomes.
We conducted a register-based nationwide cohort study with 4.7 million Danish adult citizens. All healthcare contacts to primary care and hospitals during 2018 were recorded. Clinical fragmentation indicators included number of healthcare contacts, involved providers, provider transitions, and hospital trajectories. Formal fragmentation indices assessed care concentration, dispersion, and contact sequence. The patient outcomes were potentially inappropriate medication and all-cause mortality adjusted for demographics, socioeconomic factors, and morbidity level.
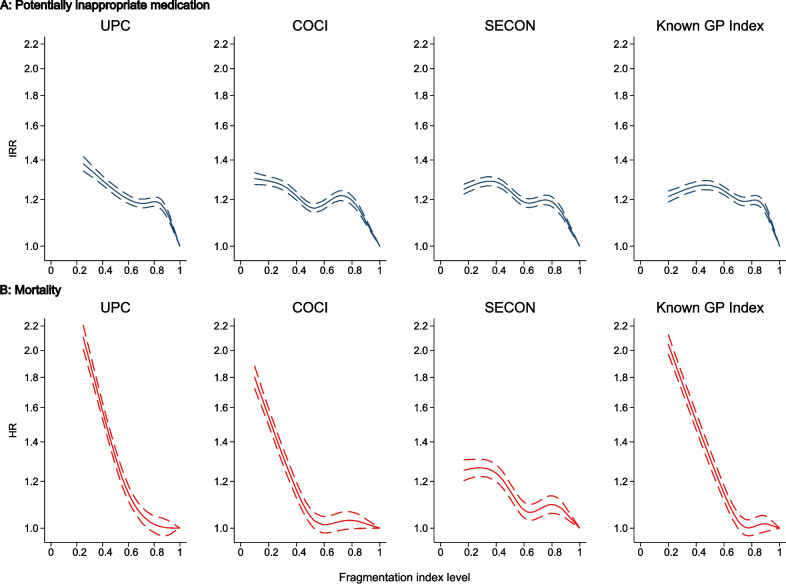
The number of involved healthcare providers, provider transitions, and hospital trajectories rose with increasing morbidity levels. Patients with 3 versus 6 conditions had a mean of 4.0 versus 6.9 involved providers and 6.6 versus 13.7 provider transitions. The proportion of contacts to the patient's own general practice remained stable across morbidity levels. High levels of care fragmentation were associated with higher rates of potentially inappropriate medication and increased mortality on all fragmentation measures after adjusting for demographic characteristics, socioeconomic factors, and morbidity. The strongest associations with potentially inappropriate medication and mortality were found for ≥ 20 contacts versus none (incidence rate ratio 2.83, 95% CI 2.77-2.90) and ≥ 20 hospital trajectories versus none (hazard ratio 10.8, 95% CI 9.48-12.4), respectively. Having less than 25% of contacts with your usual provider was associated with an incidence rate ratio of potentially inappropriate medication of 1.49 (95% CI 1.40-1.58) and a mortality hazard ratio of 2.59 (95% CI 2.36-2.84) compared with full continuity. For the associations between fragmentation measures and patient outcomes, there were no clear interactions with number of conditions.
Several clinical indicators of care fragmentation were associated with morbidity level. Care fragmentation was associated with higher rates of potentially inappropriate medication and increased mortality even when adjusting for the most important confounders. Frequent contact to the usual provider, fewer transitions, and better coordination were associated with better patient outcomes regardless of morbidity level.
患有多种疾病的患者经常使用医疗保健服务,但碎片化的护理可能导致治疗效果不佳。然而,这在全国范围内从未在医疗保健部门进行过检查。我们旨在使用各种措施量化护理碎片化,并分析其与患者结果的关联。
我们进行了一项基于登记的全国性队列研究,纳入了 470 万丹麦成年公民。记录了 2018 年期间所有初级保健和医院的医疗接触情况。临床碎片化指标包括医疗接触次数、涉及的提供者、提供者过渡和医院轨迹。正式的碎片化指数评估了护理的集中程度、分散程度和接触顺序。患者结果是经人口统计学、社会经济因素和发病水平调整后的潜在不适当药物和全因死亡率。
随着发病水平的升高,涉及的医疗保健提供者数量、提供者过渡和医院轨迹也随之增加。患有 3 种与 6 种疾病的患者平均涉及 4.0 名与 6.9 名提供者,有 6.6 次与 13.7 次提供者过渡。在发病水平上,接触患者自己的常规诊所的比例保持稳定。在调整人口统计学特征、社会经济因素和发病水平后,高水平的护理碎片化与所有碎片化指标上更高的潜在不适当药物使用率和死亡率相关。与潜在不适当药物和死亡率关联最强的是与无接触相比,接触次数≥20 次(发病率比 2.83,95%置信区间 2.77-2.90)和接触次数≥20 次的医院轨迹(风险比 10.8,95%置信区间 9.48-12.4)。与常规提供者的接触次数少于 25%相比,潜在不适当药物的发病率比为 1.49(95%置信区间 1.40-1.58),死亡率的风险比为 2.59(95%置信区间 2.36-2.84)。对于碎片化措施与患者结果之间的关联,与发病水平无关。
几种护理碎片化的临床指标与发病水平相关。即使在调整了最重要的混杂因素后,护理碎片化与更高的潜在不适当药物使用率和死亡率相关。与常规提供者的频繁接触、较少的过渡和更好的协调与更好的患者结果相关,无论发病水平如何。