Department of Medical Oncology, The Christie NHS Foundation Trust, Wilmslow Road, Manchester, M20 4BX, UK.
Division of Cancer Sciences, The University of Manchester, Manchester, UK.
Breast Cancer Res Treat. 2023 Nov;202(1):83-95. doi: 10.1007/s10549-023-07035-6. Epub 2023 Aug 16.
ER+/HER2- advanced breast cancer (ABC) with visceral crisis (VC) or impending VC (IVC) is commonly treated with chemotherapy instead of CDK4/6 inhibitors (CDK4/6i). However, there is little evidence to confirm which treatment is superior. This study compared outcomes of patients with ER+/HER2- ABC and IVC/VC treated with CDK4/6i or weekly paclitaxel.
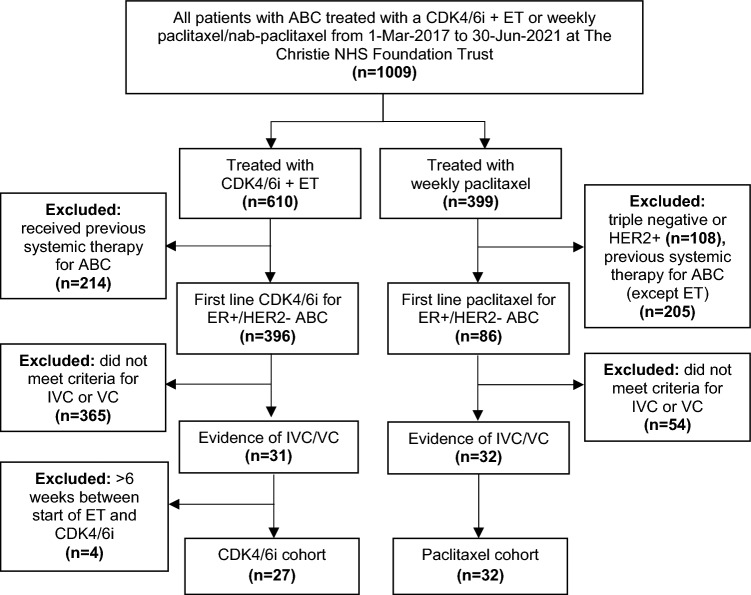
Patients with ER+/HER2- ABC receiving first line treatment at a large tertiary UK cancer centre from 1-Mar-2017 to 30-Jun-2021 were retrospectively identified. Hospital records were screened for IVC/VC affecting the liver, lungs/mediastinum, gastrointestinal tract and/or bone marrow. Baseline demographics, clinical data and survival outcomes were recorded up to 30-Jul-2022.
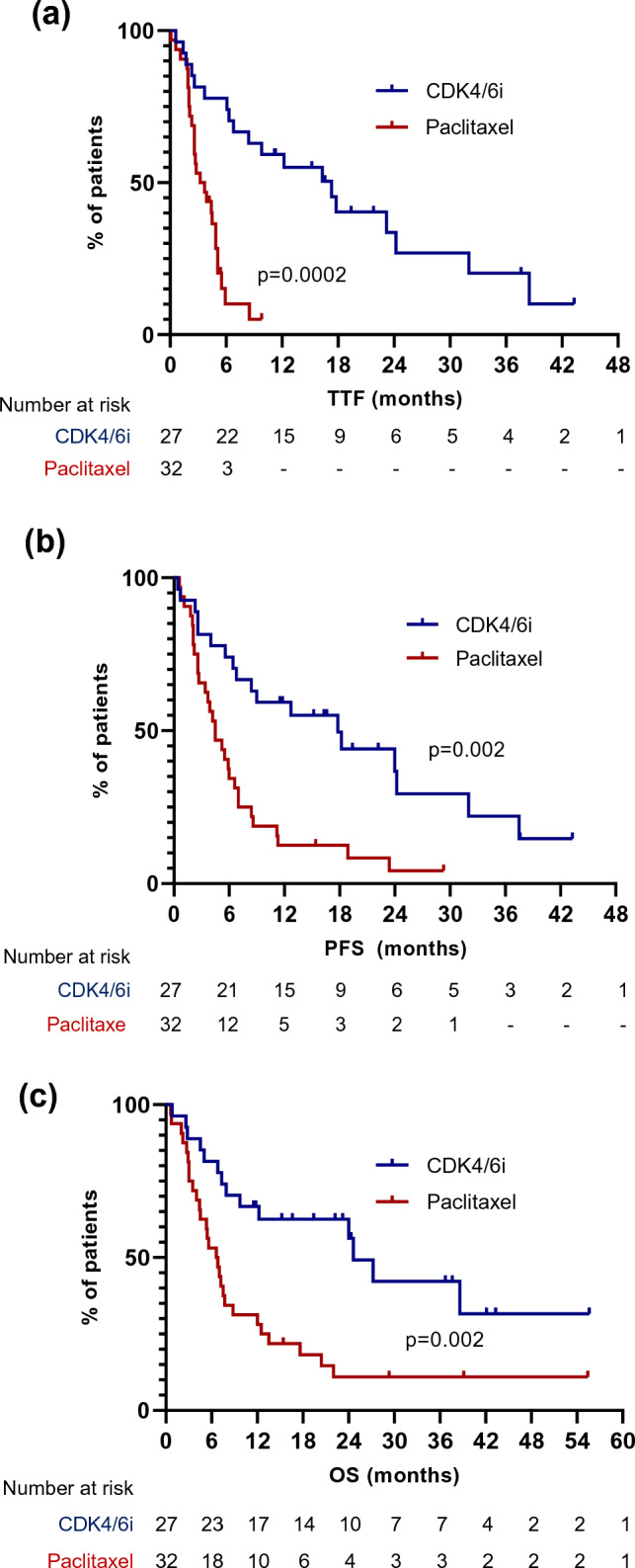
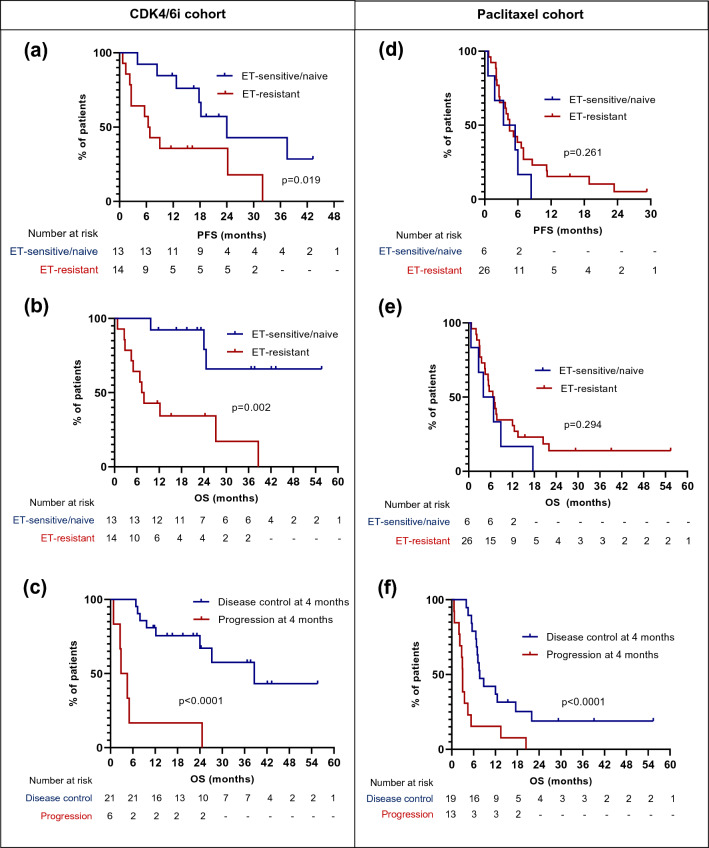
27/396 (6.8%) patients with ABC who received CDK4/6i and 32/86 (37.2%) who received paclitaxel had IVC/VC. Median time to treatment failure (TTF), progression-free survival (PFS) and overall survival (OS) were significantly longer in the CDK4/6i compared to paclitaxel cohort: TTF 17.3 vs. 3.5 months (HR 0.33, 95%CI 0.17-0.61, p = 0.0002), PFS 17.8 vs. 4.5 months (HR 0.38, 95%CI 0.21-0.67, p = 0.002), OS 24.6 vs. 6.7 months (HR 0.37, 95%CI 0.20-0.68, p = 0.002). The median time to first improvement in IVC/VC was similar in patients receiving CDK4/6i compared to paclitaxel (3.9 vs. 3.6 weeks, p = 0.773). Disease control at 4 months was not significantly different in the CDK4/6i and paclitaxel cohorts (77.8% vs. 59.4%, p = 0.168). In multivariate analysis, treatment with CDK4/6i was independently associated with a longer PFS compared to paclitaxel (HR 0.31, 95%CI 0.12-0.78, p = 0.015).
In this retrospective study, patients with ER+/HER2- ABC and IVC/VC treated with CDK4/6i had a significantly better survival compared to those treated with weekly paclitaxel. Further prospective studies that minimise possible selection bias are recommended.
对于有内脏危机(VC)或即将发生 VC(IVC)的 ER+/HER2- 晚期乳腺癌(ABC),通常采用化疗而不是 CDK4/6 抑制剂(CDK4/6i)进行治疗。然而,几乎没有证据可以证实哪种治疗方法更优越。本研究比较了接受 CDK4/6i 或每周紫杉醇治疗的 ER+/HER2- ABC 伴 IVC/VC 患者的结局。
从 2017 年 3 月 1 日至 2021 年 6 月 30 日,回顾性地从英国一家大型三级癌症中心接受一线治疗的 ER+/HER2- ABC 患者中确定了该研究的患者。筛选了影响肝脏、肺/纵隔、胃肠道和/或骨髓的 IVC/VC 的医院记录。记录了截止到 2022 年 7 月 30 日的基线人口统计学、临床数据和生存结局。
在接受 CDK4/6i 治疗的 396 例 ABC 患者中,有 27 例(6.8%)和接受紫杉醇治疗的 86 例 ABC 患者中有 32 例(37.2%)发生了 IVC/VC。与紫杉醇组相比,CDK4/6i 组的治疗失败时间(TTF)、无进展生存期(PFS)和总生存期(OS)显著更长:TTF 17.3 与 3.5 个月(HR 0.33,95%CI 0.17-0.61,p=0.0002),PFS 17.8 与 4.5 个月(HR 0.38,95%CI 0.21-0.67,p=0.002),OS 24.6 与 6.7 个月(HR 0.37,95%CI 0.20-0.68,p=0.002)。与接受紫杉醇治疗的患者相比,接受 CDK4/6i 治疗的患者首次改善 IVC/VC 的中位时间相似(3.9 与 3.6 周,p=0.773)。4 个月时的疾病控制率在 CDK4/6i 和紫杉醇组之间没有显著差异(77.8% vs. 59.4%,p=0.168)。在多变量分析中,与紫杉醇相比,CDK4/6i 治疗与较长的 PFS 相关(HR 0.31,95%CI 0.12-0.78,p=0.015)。
在这项回顾性研究中,与接受每周紫杉醇治疗的患者相比,接受 CDK4/6i 治疗的 ER+/HER2- ABC 伴 IVC/VC 的患者具有显著更好的生存结局。建议进行进一步的前瞻性研究,以最大限度地减少可能的选择偏倚。